
Crohn’s Disease-Associated and Cryptoglandular Fistulas: Differences and Similarities
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
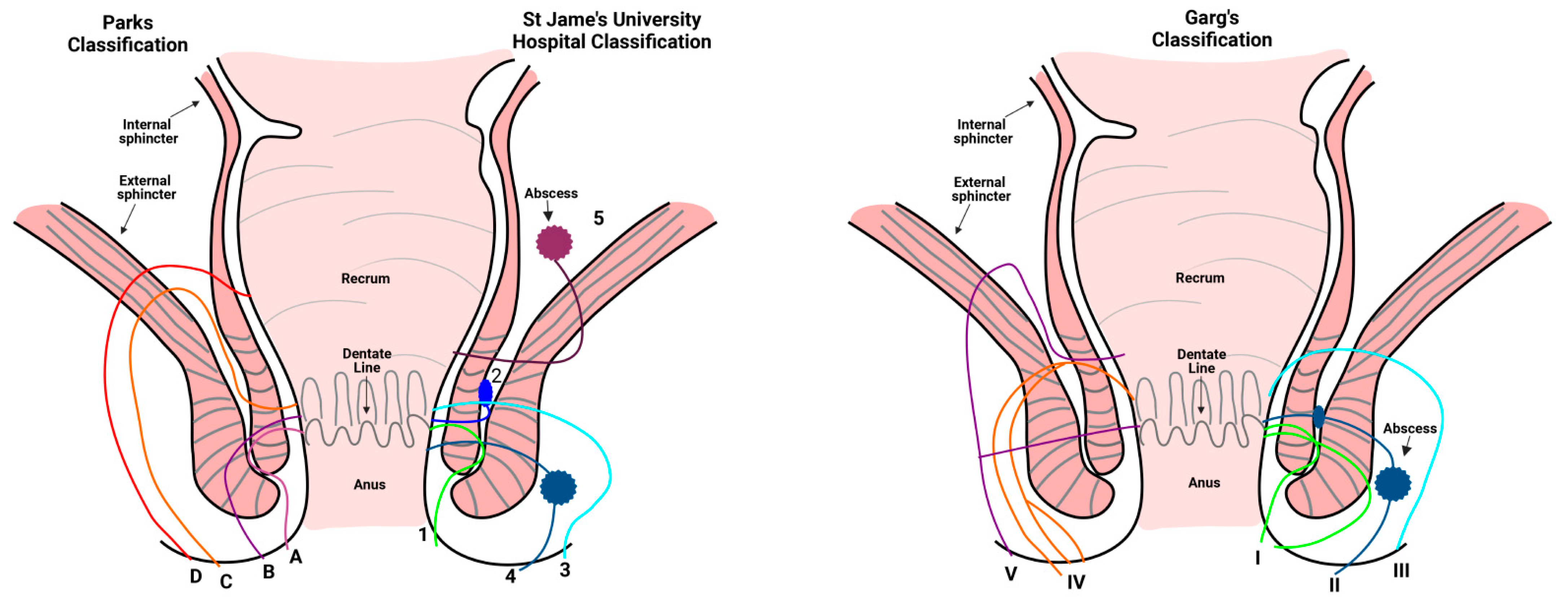
2. Classification of Perianal Fistulas
3. Epidemiology
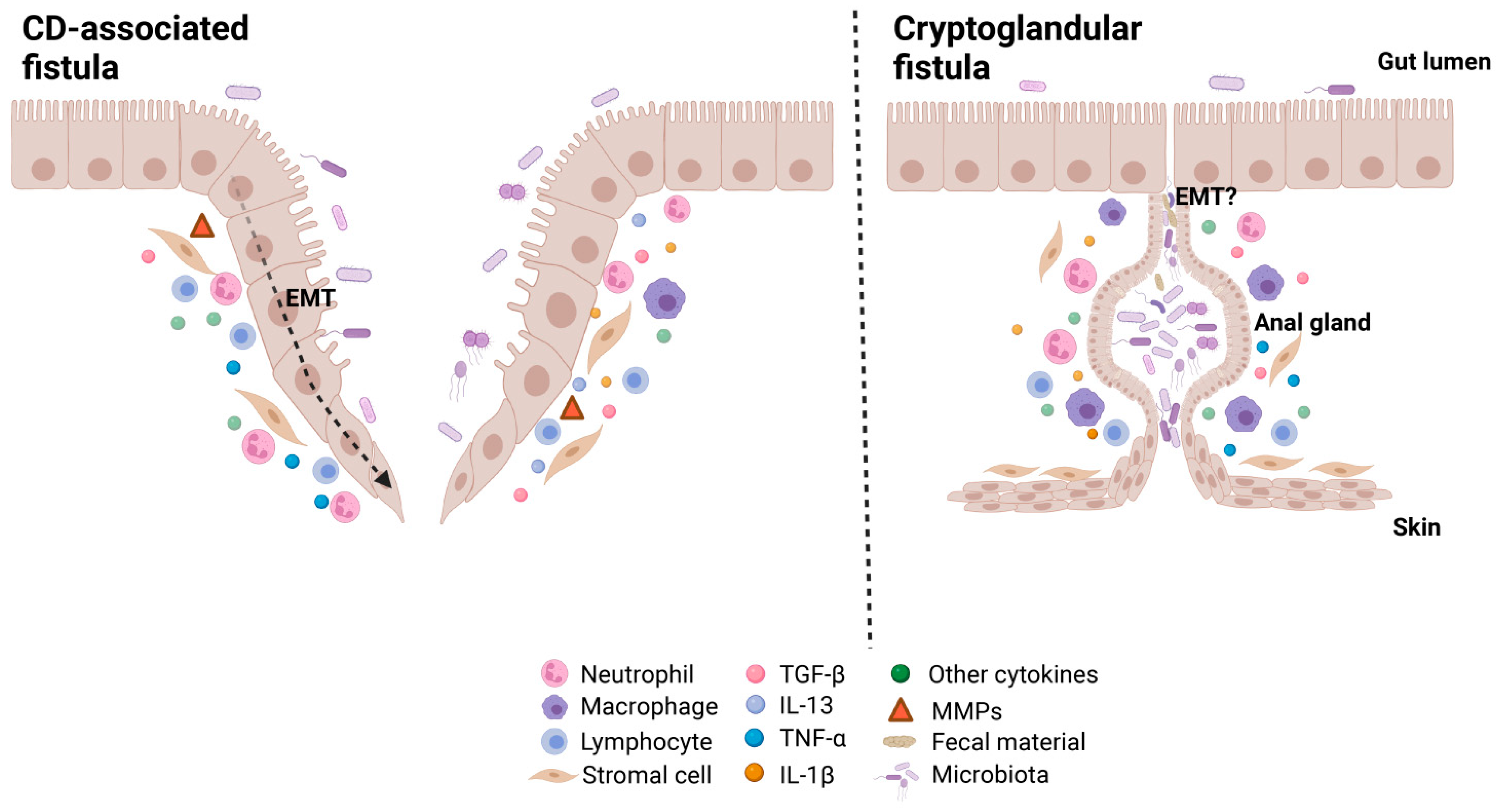
4. Pathogenesis
4.1. Anal Gland Inflammation
4.2. Intestinal Inflammation
4.3. Epithelial-Mesenchymal Transition
4.4. Microbiota
5. Treatment
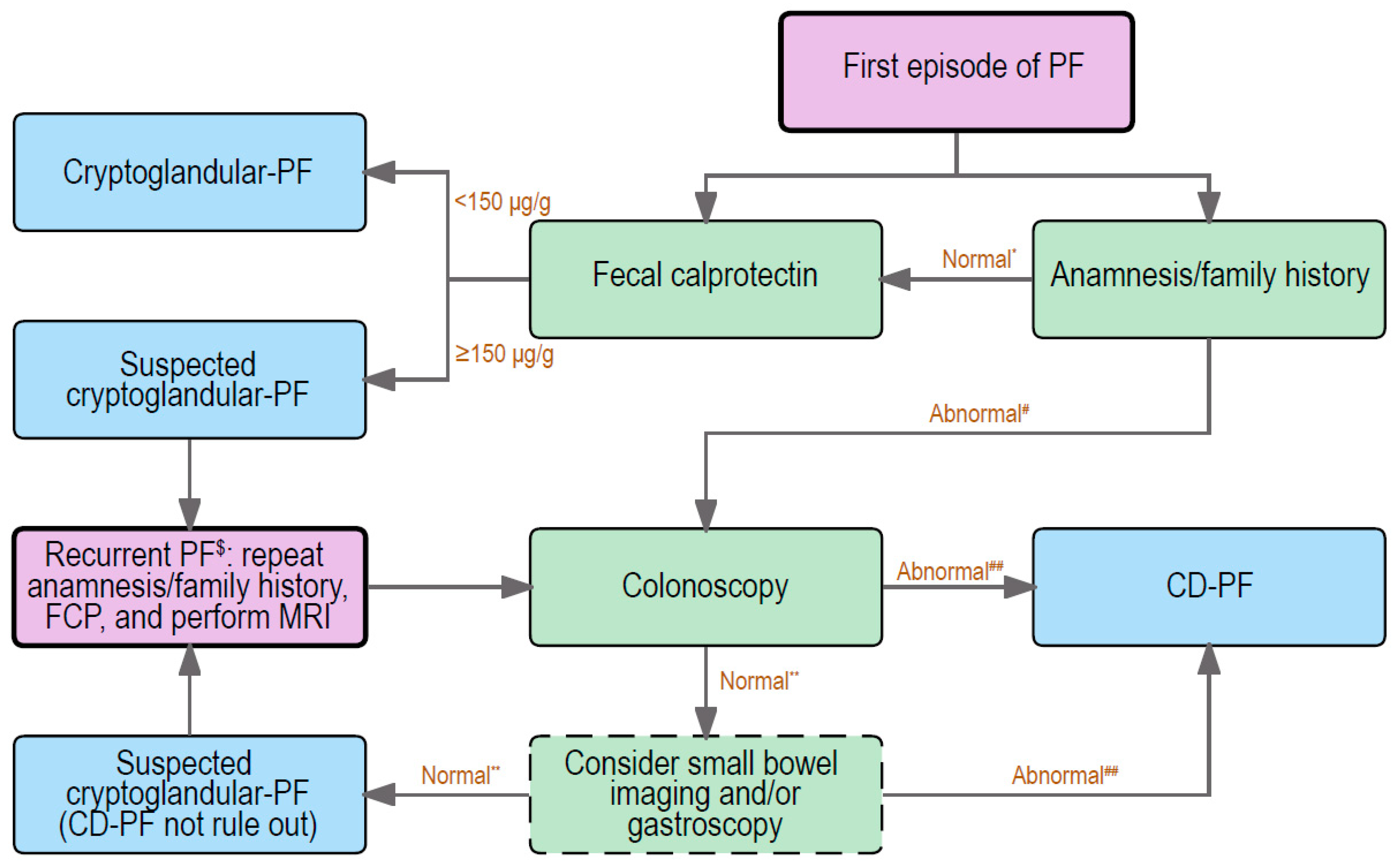
6. Distinction between Cryptoglandular and CD-Associated Fistulas: Clinical Practice
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Miguel Criado, J.; del Salto, L.G.; Rivas, P.F.; del Hoyo, L.F.; Velasco, L.G.; de las Vacas, M.I.; Marco Sanz, A.G.; Paradela, M.M.; Moreno, E.F. MR imaging evaluation of perianal fistulas: Spectrum of imaging features. Radiogr. A Rev. Publ. Radiol. Soc. N. Am. Inc 2012, 32, 175–194. [Google Scholar] [CrossRef]
- Vogel, J.D.; Johnson, E.K.; Morris, A.M.; Paquette, I.M.; Saclarides, T.J.; Feingold, D.L.; Steele, S.R. Clinical Practice Guideline for the Management of Anorectal Abscess, Fistula-in-Ano, and Rectovaginal Fistula. Dis. Colon Rectum 2016, 59, 1117–1133. [Google Scholar] [CrossRef] [PubMed]
- Whiteford, M.H. Perianal abscess/fistula disease. Clin. Colon Rectal Surg. 2007, 20, 102–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendrickson, B.A.; Gokhale, R.; Cho, J.H. Clinical aspects and pathophysiology of inflammatory bowel disease. Clin. Microbiol. Rev. 2002, 15, 79–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottgens, K.W.; Jeuring, S.F.; Sturkenboom, R.; Romberg-Camps, M.J.; Oostenbrug, L.E.; Jonkers, D.M.; Stassen, L.P.; Masclee, A.A.; Pierik, M.J.; Breukink, S.O. Time trends in the epidemiology and outcome of perianal fistulizing Crohn’s disease in a population-based cohort. Eur. J. Gastroenterol. Hepatol. 2017, 29, 595–601. [Google Scholar] [CrossRef]
- Mizushima, T.; Ota, M.; Fujitani, Y.; Kanauchi, Y.; Iwakiri, R. Diagnostic Features of Perianal Fistula in Patients With Crohn’s Disease: Analysis of a Japanese Claims Database. Crohn’s Colitis 360 2021, 3, otab055. [Google Scholar] [CrossRef]
- Sica, G.S.; Di Carlo, S.; Tema, G.; Montagnese, F.; Del Vecchio Blanco, G.; Fiaschetti, V.; Maggi, G.; Biancone, L. Treatment of peri-anal fistula in Crohn’s disease. World J. Gastroenterol. 2014, 20, 13205–13210. [Google Scholar] [CrossRef]
- Limura, E.; Giordano, P. Modern management of anal fistula. World J. Gastroenterol. 2015, 21, 12–20. [Google Scholar] [CrossRef]
- Kotze, P.G.; Shen, B.; Lightner, A.; Yamamoto, T.; Spinelli, A.; Ghosh, S.; Panaccione, R. Modern management of perianal fistulas in Crohn’s disease: Future directions. Gut 2018, 67, 1181–1194. [Google Scholar] [CrossRef]
- Bell, S.J.; Williams, A.B.; Wiesel, P.; Wilkinson, K.; Cohen, R.C.; Kamm, M.A. The clinical course of fistulating Crohn’s disease. Aliment Pharm. 2003, 17, 1145–1151. [Google Scholar] [CrossRef]
- Marzo, M.; Felice, C.; Pugliese, D.; Andrisani, G.; Mocci, G.; Armuzzi, A.; Guidi, L. Management of perianal fistulas in Crohn’s disease: An up-to-date review. World J. Gastroenterol. 2015, 21, 1394–1403. [Google Scholar] [CrossRef] [PubMed]
- Mei, Z.; Wang, Q.; Zhang, Y.; Liu, P.; Ge, M.; Du, P.; Yang, W.; He, Y. Risk Factors for Recurrence after anal fistula surgery: A meta-analysis. Int. J. Surg. 2019, 69, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Parks, A.G. Pathogenesis and treatment of fistuila-in-ano. Br. Med. J. 1961, 1, 463–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scharl, M.; Rogler, G. Pathophysiology of fistula formation in Crohn’s disease. World J. Gastrointest. Pathophysiol. 2014, 5, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Chin Koon Siw, K.; Engel, J.; Visva, S.; Mallick, R.; Hart, A.; de Buck van Overstraeten, A.; McCurdy, J.D. Strategies to Distinguish Perianal Fistulas Related to Crohn’s Disease From Cryptoglandular Disease: Systematic Review With Meta-Analysis. Inflamm. Bowel Dis. 2022, 28, 1363–1374. [Google Scholar] [CrossRef]
- Parks, A.G.; Gordon, P.H.; Hardcastle, J.D. A classification of fistula-in-ano. Br. J. Surg. 1976, 63, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Steele, S.R.; Kumar, R.; Feingold, D.L.; Rafferty, J.L.; Buie, W.D. Practice parameters for the management of perianal abscess and fistula-in-ano. Dis. Colon Rectum 2011, 54, 1465–1474. [Google Scholar] [CrossRef]
- Sahni, V.A.; Ahmad, R.; Burling, D. Which method is best for imaging of perianal fistula? Abdom Imaging 2008, 33, 26–30. [Google Scholar] [CrossRef]
- Morris, J.; Spencer, J.A.; Ambrose, N.S. MR imaging classification of perianal fistulas and its implications for patient management. Radiographics 2000, 20, 623–635, discussion 635–627. [Google Scholar] [CrossRef]
- Garg, P. Garg Classification for Anal Fistulas: Is It Better than Existing Classifications?—A Review. Indian J. Surg. 2018, 80, 606–608. [Google Scholar] [CrossRef]
- Garg, P. Comparing existing classifications of fistula-in-ano in 440 operated patients: Is it time for a new classification? A Retrospective Cohort Study. Int. J. Surg. 2017, 42, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Zanotti, C.; Martinez-Puente, C.; Pascual, I.; Pascual, M.; Herreros, D.; Garcia-Olmo, D. An assessment of the incidence of fistula-in-ano in four countries of the European Union. Int. J. Color. Dis. 2007, 22, 1459–1462. [Google Scholar] [CrossRef]
- Garcia-Olmo, D.; Van Assche, G.; Tagarro, I.; Diez, M.C.; Richard, M.P.; Khalid, J.M.; van Dijk, M.; Bennett, D.; Hokkanen, S.R.K.; Panes, J. Prevalence of Anal Fistulas in Europe: Systematic Literature Reviews and Population-Based Database Analysis. Adv 2019, 36, 3503–3518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, R. Anorectal abscess fistula: What do we know? Surg. Clin North Am 2002, 82, 1139–1151, v–vi. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yang, W.; Huang, Z.; Mei, Z.; Yang, D.; Wu, H.; Wang, Q. Clinical characteristics and risk factors for recurrence of anal fistula patients. Zhonghua Wei Chang Wai Ke Za Zhi 2016, 19, 1370–1374. [Google Scholar]
- Sahnan, K.; Askari, A.; Adegbola, S.O.; Tozer, P.J.; Phillips, R.K.S.; Hart, A.; Faiz, O.D. Natural history of anorectal sepsis. Br. J. Surg. 2017, 104, 1857–1865. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Loftus, E.V., Jr.; Tremaine, W.J.; Panaccione, R.; Harmsen, W.S.; Zinsmeister, A.R.; Sandborn, W.J. The natural history of fistulizing Crohn’s disease in Olmsted County, Minnesota. Gastroenterology 2002, 122, 875–880. [Google Scholar] [CrossRef]
- Eglinton, T.W.; Barclay, M.L.; Gearry, R.B.; Frizelle, F.A. The spectrum of perianal Crohn’s disease in a population-based cohort. Dis. Colon Rectum 2012, 55, 773–777. [Google Scholar] [CrossRef]
- Hellers, G.; Bergstrand, O.; Ewerth, S.; Holmstrom, B. Occurrence and outcome after primary treatment of anal fistulae in Crohn’s disease. Gut 1980, 21, 525–527. [Google Scholar] [CrossRef] [Green Version]
- Mak, W.Y.; Mak, O.S.; Lee, C.K.; Tang, W.; Leung, W.K.; Wong, M.T.L.; Sze, A.S.F.; Li, M.; Leung, C.M.; Lo, F.H.; et al. Significant Medical and Surgical Morbidity in Perianal Crohn’s Disease: Results from a Territory-Wide Study. J. Crohns Colitis 2018, 12, 1392–1398. [Google Scholar] [CrossRef]
- Park, S.H.; Aniwan, S.; Scott Harmsen, W.; Tremaine, W.J.; Lightner, A.L.; Faubion, W.A.; Loftus, E.V. Update on the Natural Course of Fistulizing Perianal Crohn’s Disease in a Population-Based Cohort. Inflamm. Bowel Dis. 2019, 25, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Zeitz, J.; Fournier, N.; Labenz, C.; Biedermann, L.; Frei, P.; Misselwitz, B.; Scharl, S.; Vavricka, S.R.; Sulz, M.C.; Fried, M.; et al. Risk Factors for the Development of Fistulae and Stenoses in Crohn Disease Patients in the Swiss Inflammatory Bowel Disease Cohort. Inflamm. Intest Dis. 2017, 1, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Chun, J.; Im, J.P.; Kim, J.W.; Lee, K.L.; Choi, C.H.; Kim, H.; Cheon, J.H.; Ye, B.D.; Kim, Y.H.; Kim, Y.S.; et al. Association of Perianal Fistulas with Clinical Features and Prognosis of Crohn’s Disease in Korea: Results from the CONNECT Study. Gut Liver 2018, 12, 544–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sainio, P. Fistula-in-ano in a defined population. Incidence and epidemiological aspects. Ann. Chir. Gynaecol. 1984, 73, 219–224. [Google Scholar]
- Eisenhammer, S. Emergency fistulectomy of the acute primary anorectal cryptoglandular intermuscular abscess-fistula in ano. S. Afr. J. Surg. 1985, 23, 1–7. [Google Scholar]
- Emile, S.H.; Elfeki, H.; Abdelnaby, M. A systematic review of the management of anal fistula in infants. Tech. Coloproctol. 2016, 20, 735–744. [Google Scholar] [CrossRef]
- Hamadani, A.; Haigh, P.I.; Liu, I.L.; Abbas, M.A. Who is at risk for developing chronic anal fistula or recurrent anal sepsis after initial perianal abscess? Dis. Colon Rectum 2009, 52, 217–221. [Google Scholar] [CrossRef]
- Seow-Choen, F.; Ho, J.M. Histoanatomy of anal glands. Dis. Colon Rectum 1994, 37, 1215–1218. [Google Scholar] [CrossRef]
- Goligher, J.C.; Ellis, M.; Pissidis, A.G. A critique of anal glandular infection in the aetiology and treatment of idiopathic anorectal abscesses and fistulas. Br. J. Surg. 1967, 54, 977–983. [Google Scholar] [CrossRef]
- Mitalas, L.E.; van Onkelen, R.S.; Monkhorst, K.; Zimmerman, D.D.; Gosselink, M.P.; Schouten, W.R. Identification of epithelialization in high transsphincteric fistulas. Tech. Coloproctol. 2012, 16, 113–117. [Google Scholar] [CrossRef] [Green Version]
- American Gastroenterological Association. American Gastroenterological Association medical position statement: Perianal Crohn’s disease. Gastroenterology 2003, 125, 1503–1507. [Google Scholar] [CrossRef]
- Kelley, K.A.; Kaur, T.; Tsikitis, V.L. Perianal Crohn’s disease: Challenges and solutions. Clin. Exp. Gastroenterol. 2017, 10, 39–46. [Google Scholar] [CrossRef] [PubMed]
- McColl, I. The comparative anatomy and pathology of anal glands. Arris and Gale lecture delivered at the Royal College of Surgeons of England on 25th February 1965. Ann. R Coll. Surg. Engl. 1967, 40, 36–67. [Google Scholar]
- Sordo-Mejia, R.; Gaertner, W.B. Multidisciplinary and evidence-based management of fistulizing perianal Crohn’s disease. World J. Gastrointest. Pathophysiol. 2014, 5, 239–251. [Google Scholar] [CrossRef]
- Zhang, M.; Sun, K.; Wu, Y.; Yang, Y.; Tso, P.; Wu, Z. Interactions between Intestinal Microbiota and Host Immune Response in Inflammatory Bowel Disease. Front Immunol. 2017, 8, 942. [Google Scholar] [CrossRef] [Green Version]
- Petagna, L.; Antonelli, A.; Ganini, C.; Bellato, V.; Campanelli, M.; Divizia, A.; Efrati, C.; Franceschilli, M.; Guida, A.M.; Ingallinella, S.; et al. Pathophysiology of Crohn’s disease inflammation and recurrence. Biol. Direct. 2020, 15, 23. [Google Scholar] [CrossRef] [PubMed]
- Bruckner, R.S.; Spalinger, M.R.; Barnhoorn, M.C.; Feakins, R.; Fuerst, A.; Jehle, E.C.; Rickenbacher, A.; Turina, M.; Niechcial, A.; Lang, S.; et al. Contribution of CD3+CD8- and CD3+CD8+ T Cells to TNF-alpha Overexpression in Crohn Disease-Associated Perianal Fistulas and Induction of Epithelial-Mesenchymal Transition in HT-29 Cells. Inflamm. Bowel Dis. 2021, 27, 538–549. [Google Scholar] [CrossRef]
- Maggi, L.; Capone, M.; Giudici, F.; Santarlasci, V.; Querci, V.; Liotta, F.; Ficari, F.; Maggi, E.; Tonelli, F.; Annunziato, F.; et al. CD4+CD161+ T lymphocytes infiltrate Crohn’s disease-associated perianal fistulas and are reduced by anti-TNF-alpha local therapy. Int. Arch. Allergy Immunol 2013, 161, 81–86. [Google Scholar] [CrossRef]
- van Unen, V.; Li, N.; Molendijk, I.; Temurhan, M.; Hollt, T.; van der Meulen-de Jong, A.E.; Verspaget, H.W.; Mearin, M.L.; Mulder, C.J.; van Bergen, J.; et al. Mass Cytometry of the Human Mucosal Immune System Identifies Tissue- and Disease-Associated Immune Subsets. Immunity 2016, 44, 1227–1239. [Google Scholar] [CrossRef] [Green Version]
- Becker, M.; de Krijger, M.; Bemelman, W.; de Jonge, W.; Buskens, C.; Wildenberg, M.; Dige, S.T. DOP24 Crohn’s Disease fistula show skewed lymphoid/myeloid balance, altered myeloid cell profiles and high TNF-α expression. J. Crohn’s Colitis 2021, 15, S062–S063. [Google Scholar] [CrossRef]
- van Onkelen, R.S.; Gosselink, M.P.; van Meurs, M.; Melief, M.J.; Schouten, W.R.; Laman, J.D. Pro-inflammatory cytokines in cryptoglandular anal fistulas. Tech. Coloproctol. 2016, 20, 619–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratto, C.; Litta, F.; Lucchetti, D.; Parello, A.; Boninsegna, A.; Arena, V.; Donisi, L.; Calapa, F.; Sgambato, A. Immunopathological characterization of cryptoglandular anal fistula: A pilot study investigating its pathogenesis. Color. Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2016, 18, O436–O444. [Google Scholar] [CrossRef]
- Barnhoorn, M.; Schepers, K.; Verspaget, H.; Fibbe, W.; Hawinkels, L.; van Pel, M.; van der Meulen-de Jong, A. P040 The cytokine milieu in patients with inflammatory bowel disease impacts the phenotype of mesenchymal stromal cells. J. Crohn’s Colitis 2019, 13, S106–S107. [Google Scholar] [CrossRef]
- Chen, T.; You, Y.; Jiang, H.; Wang, Z.Z. Epithelial-mesenchymal transition (EMT): A biological process in the development, stem cell differentiation, and tumorigenesis. J. Cell Physiol. 2017, 232, 3261–3272. [Google Scholar] [CrossRef] [PubMed]
- Bataille, F.; Rohrmeier, C.; Bates, R.; Weber, A.; Rieder, F.; Brenmoehl, J.; Strauch, U.; Farkas, S.; Furst, A.; Hofstadter, F.; et al. Evidence for a role of epithelial mesenchymal transition during pathogenesis of fistulae in Crohn’s disease. Inflamm. Bowel Dis. 2008, 14, 1514–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scharl, M.; Weber, A.; Furst, A.; Farkas, S.; Jehle, E.; Pesch, T.; Kellermeier, S.; Fried, M.; Rogler, G. Potential role for SNAIL family transcription factors in the etiology of Crohn’s disease-associated fistulae. Inflamm. Bowel Dis. 2011, 17, 1907–1916. [Google Scholar] [CrossRef]
- Scharl, M.; Frei, S.; Pesch, T.; Kellermeier, S.; Arikkat, J.; Frei, P.; Fried, M.; Weber, A.; Jehle, E.; Ruhl, A.; et al. Interleukin-13 and transforming growth factor beta synergise in the pathogenesis of human intestinal fistulae. Gut 2013, 62, 63–72. [Google Scholar] [CrossRef]
- Frei, S.M.; Pesch, T.; Lang, S.; Weber, A.; Jehle, E.; Vavricka, S.R.; Fried, M.; Rogler, G.; Scharl, M. A role for tumor necrosis factor and bacterial antigens in the pathogenesis of Crohn’s disease-associated fistulae. Inflamm. Bowel Dis. 2013, 19, 2878–2887. [Google Scholar] [CrossRef]
- Kirkegaard, T.; Hansen, A.; Bruun, E.; Brynskov, J. Expression and localisation of matrix metalloproteinases and their natural inhibitors in fistulae of patients with Crohn’s disease. Gut 2004, 53, 701–709. [Google Scholar] [CrossRef] [Green Version]
- Glassner, K.L.; Abraham, B.P.; Quigley, E.M.M. The microbiome and inflammatory bowel disease. J. Allergy Clin. Immunol. 2020, 145, 16–27. [Google Scholar] [CrossRef] [Green Version]
- Haac, B.E.; Palmateer, N.C.; Seaton, M.E.; Van, Y.R.; Fraser, C.M.; Bafford, A.C. A Distinct Gut Microbiota Exists Within Crohn’s Disease-Related Perianal Fistulae. J. Surg. Res. 2019, 242, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Tozer, P.J.; Rayment, N.; Hart, A.L.; Daulatzai, N.; Murugananthan, A.U.; Whelan, K.; Phillips, R.K. What role do bacteria play in persisting fistula formation in idiopathic and Crohn’s anal fistula? Color. Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2015, 17, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Radlmayr, M.; Torok, H.P.; Martin, K.; Folwaczny, C. The c-insertion mutation of the NOD2 gene is associated with fistulizing and fibrostenotic phenotypes in Crohn’s disease. Gastroenterology 2002, 122, 2091–2092. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Wang, Q.; Mei, Z. Preliminary study on the pathogenesis of anal fistula. medRxiv 2021, 2021.2004.2015.21254769. [Google Scholar] [CrossRef]
- Eykyn, S.J.; Grace, R.H. The relevance of microbiology in the management of anorectal sepsis. Ann. R Coll Surg. Engl 1986, 68, 237–239. [Google Scholar]
- Toyonaga, T.; Matsushima, M.; Tanaka, Y.; Shimojima, Y.; Matsumura, N.; Kannyama, H.; Nozawa, M.; Hatakeyama, T.; Suzuki, K.; Yanagita, K.; et al. Microbiological analysis and endoanal ultrasonography for diagnosis of anal fistula in acute anorectal sepsis. Int. J. Color. Dis. 2007, 22, 209–213. [Google Scholar] [CrossRef]
- Leung, E.; McArdle, K.; Yazbek-Hanna, M. Pus swabs in incision and drainage of perianal abscesses: What is the point? World J. Surg. 2009, 33, 2448–2451. [Google Scholar] [CrossRef]
- Xu, R.W.; Tan, K.K.; Chong, C.S. Bacteriological study in perianal abscess is not useful and not cost-effective. ANZ J. Surg. 2016, 86, 782–784. [Google Scholar] [CrossRef]
- van Onkelen, R.S.; Mitalas, L.E.; Gosselink, M.P.; van Belkum, A.; Laman, J.D.; Schouten, W.R. Assessment of microbiota and peptidoglycan in perianal fistulas. Diagn. Microbiol. Infect. Dis. 2013, 75, 50–54. [Google Scholar] [CrossRef]
- Spinelli, A.; Armuzzi, A.; Ciccocioppo, R.; Danese, S.; Gionchetti, P.; Luglio, G.; Orlando, A.; Rispo, A.; Rizzello, F.; Sofo, L.; et al. Management of patients with complex perianal fistulas in Crohn’s disease: Optimal patient flow in the Italian clinical reality. Dig. Liver Dis. 2020, 52, 506–515. [Google Scholar] [CrossRef]
- Yarur, A.J.; Kanagala, V.; Stein, D.J.; Czul, F.; Quintero, M.A.; Agrawal, D.; Patel, A.; Best, K.; Fox, C.; Idstein, K.; et al. Higher infliximab trough levels are associated with perianal fistula healing in patients with Crohn’s disease. Aliment Pharm. 2017, 45, 933–940. [Google Scholar] [CrossRef] [Green Version]
- Adegbola, S.O.; Sarafian, M.; Sahnan, K.; Pechlivanis, A.; Phillips, R.K.S.; Warusavitarne, J.; Faiz, O.; Haddow, J.; Knowles, C.; Tozer, P.; et al. Lack of anti-TNF drugs levels in fistula tissue—a reason for nonresponse in Crohn’s perianal fistulating disease? Eur. J. Gastroenterol. Hepatol. 2022, 34, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Chudy-Onwugaje, K.O.; Christian, K.E.; Farraye, F.A.; Cross, R.K. A State-of-the-Art Review of New and Emerging Therapies for the Treatment of IBD. Inflamm. Bowel Dis. 2019, 25, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Schwartz, D.; Danese, S.; Rubin, D.T.; Lissoos, T.W.; Xu, J.; Lasch, K. Efficacy of Vedolizumab in Fistulising Crohn’s Disease: Exploratory Analyses of Data from GEMINI 2. J. Crohn’s Colitis 2018, 12, 621–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attauabi, M.; Burisch, J.; Seidelin, J.B. Efficacy of Ustekinumab for Active Perianal Fistulizing Crohn Disease: A Double-Center Cohort Study. Inflamm. Bowel Dis. 2021, 27, e37–e38. [Google Scholar] [CrossRef] [PubMed]
- de Groof, E.J.; Cabral, V.N.; Buskens, C.J.; Morton, D.G.; Hahnloser, D.; Bemelman, W.A.; the Research Committee of the European Society of Coloproctology. Systematic review of evidence and consensus on perianal fistula: An analysis of national and international guidelines. Color. Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2016, 18, O119–O134. [Google Scholar] [CrossRef]
- Ommer, A.; Herold, A.; Berg, E.; Furst, A.; Sailer, M.; Schiedeck, T. Cryptoglandular anal fistulas. Dtsch Arztebl Int. 2011, 108, 707–713. [Google Scholar] [CrossRef]
- van der Hagen, S.J.; Baeten, C.G.; Soeters, P.B.; Beets-Tan, R.G.; Russel, M.G.; van Gemert, W.G. Staged mucosal advancement flap for the treatment of complex anal fistulas: Pretreatment with noncutting Setons and in case of recurrent multiple abscesses a diverting stoma. Color. Dis. 2005, 7, 513–518. [Google Scholar] [CrossRef]
- Stellingwerf, M.E.; van Praag, E.M.; Tozer, P.J.; Bemelman, W.A.; Buskens, C.J. Systematic review and meta-analysis of endorectal advancement flap and ligation of the intersphincteric fistula tract for cryptoglandular and Crohn’s high perianal fistulas. BJS Open 2019, 3, 231–241. [Google Scholar] [CrossRef]
- Rojanasakul, A. LIFT procedure: A simplified technique for fistula-in-ano. Tech. Coloproctol. 2009, 13, 237–240. [Google Scholar] [CrossRef]
- Yassin, N.A.; Hammond, T.M.; Lunniss, P.J.; Phillips, R.K. Ligation of the intersphincteric fistula tract in the management of anal fistula. A systematic review. Color. Dis. 2013, 15, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Schwandner, O. Video-assisted anal fistula treatment (VAAFT) combined with advancement flap repair in Crohn’s disease. Tech. Coloproctol. 2013, 17, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, A.; Fiebig, A.; Krawczak, M. Five years of experience with the FiLaC laser for fistula-in-ano management: Long-term follow-up from a single institution. Tech. Coloproctol. 2017, 21, 269–276. [Google Scholar] [CrossRef] [Green Version]
- Elfeki, H.; Shalaby, M.; Emile, S.H.; Sakr, A.; Mikael, M.; Lundby, L. A systematic review and meta-analysis of the safety and efficacy of fistula laser closure. Tech. Coloproctol. 2020, 24, 265–274. [Google Scholar] [CrossRef]
- Wewer, M.D.; Zhao, M.; Nordholm-Carstensen, A.; Weimers, P.; Seidelin, J.B.; Burisch, J. The Incidence and Disease Course of Perianal Crohn’s Disease: A Danish Nationwide Cohort Study, 1997-2015. J. Crohns Colitis 2021, 15, 5–13. [Google Scholar] [CrossRef]
- Song, E.M.; Lee, H.S.; Kim, Y.J.; Oh, E.H.; Ham, N.S.; Kim, J.; Hwang, S.W.; Park, S.H.; Yang, D.H.; Ye, B.D.; et al. Incidence and Outcomes of Perianal Disease in an Asian Population with Crohn’s Disease: A Nationwide Population-Based Study. Dig. Dis. Sci. 2020, 65, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Lansdorp, C.A.; Buskens, C.J.; Gecse, K.B.; Lowenberg, M.; Stoker, J.; Bemelman, W.A.; D’Haens, G.; van Hulst, R.A. Hyperbaric oxygen therapy for the treatment of perianal fistulas in 20 patients with Crohn’s disease: Results of the HOT-TOPIC trial after 1-year follow-up. United Eur. Gastroenterol. J. 2022, 10, 160–168. [Google Scholar] [CrossRef]
- Meima-van Praag, E.M.; van Rijn, K.L.; Wasmann, K.; Snijder, H.J.; Stoker, J.; D’Haens, G.R.; Gecse, K.B.; Gerhards, M.F.; Jansen, J.M.; Dijkgraaf, M.G.W.; et al. Short-term anti-TNF therapy with surgical closure versus anti-TNF therapy in the treatment of perianal fistulas in Crohn’s disease (PISA-II): A patient preference randomised trial. Lancet Gastroenterol. Hepatol. 2022, 7, 617–626. [Google Scholar] [CrossRef]
- Barnhoorn, M.C.; Wasser, M.; Roelofs, H.; Maljaars, P.W.J.; Molendijk, I.; Bonsing, B.A.; Oosten, L.E.M.; Dijkstra, G.; van der Woude, C.J.; Roelen, D.L.; et al. Long-term evaluation of allogeneic bone marrow-derived mesenchymal stromal cell therapy for Crohn’s disease perianal fistulas. J. Crohn’s Colitis 2020, 14, 64–70. [Google Scholar] [CrossRef]
- Panes, J.; Garcia-Olmo, D.; Van Assche, G.; Colombel, J.F.; Reinisch, W.; Baumgart, D.C.; Dignass, A.; Nachury, M.; Ferrante, M.; Kazemi-Shirazi, L.; et al. Expanded allogeneic adipose-derived mesenchymal stem cells (Cx601) for complex perianal fistulas in Crohn’s disease: A phase 3 randomised, double-blind controlled trial. Lancet 2016, 388, 1281–1290. [Google Scholar] [CrossRef]
- Panes, J.; Garcia-Olmo, D.; Van Assche, G.; Colombel, J.F.; Reinisch, W.; Baumgart, D.C.; Dignass, A.; Nachury, M.; Ferrante, M.; Kazemi-Shirazi, L.; et al. Long-term Efficacy and Safety of Stem Cell Therapy (Cx601) for Complex Perianal Fistulas in Patients With Crohn’s Disease. Gastroenterology 2018, 154, 1334–1342.e1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagaishi, K.; Arimura, Y.; Fujimiya, M. Stem cell therapy for inflammatory bowel disease. J. Gastroenterol. 2015, 50, 280–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molendijk, I.; Bonsing, B.A.; Roelofs, H.; Peeters, K.C.; Wasser, M.N.; Dijkstra, G.; van der Woude, C.J.; Duijvestein, M.; Veenendaal, R.A.; Zwaginga, J.J.; et al. Allogeneic Bone Marrow-Derived Mesenchymal Stromal Cells Promote Healing of Refractory Perianal Fistulas in Patients With Crohn’s Disease. Gastroenterology 2015, 149, 918–927.e916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsch, R.D.; Keung, C.; Con, D.; Vasudevan, A.; Van Langenberg, D.R.; Niewiadomski, O. Direct health care costs of managing perianal Crohn’s Disease in a population based cohort. Scand J. Gastroenterol. 2022, 57, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.C.; Furlano, R.I.; Jick, S.S.; Meier, C.R. Inflammatory Bowel Disease and the Risk of Autoimmune Diseases. J. Crohn’s Colitis 2016, 10, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Forabosco, P.; Bouzigon, E.; Ng, M.Y.; Hermanowski, J.; Fisher, S.A.; Criswell, L.A.; Lewis, C.M. Meta-analysis of genome-wide linkage studies across autoimmune diseases. Eur. J. Hum Genet 2009, 17, 236–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moller, F.T.; Andersen, V.; Wohlfahrt, J.; Jess, T. Familial risk of inflammatory bowel disease: A population-based cohort study 1977-2011. Am J. Gastroenterol. 2015, 110, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.Y.; Bessissow, T. Does Familial IBD Have its Own Signature? J. Crohns Colitis 2018, 12, 515–516. [Google Scholar] [CrossRef] [Green Version]
- Gecse, K.; Khanna, R.; Stoker, J.; Jenkins, J.T.; Gabe, S.; Hahnloser, D.; D’Haens, G. Fistulizing Crohn’s disease: Diagnosis and management. United Eur. Gastroenterol. J. 2013, 1, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Buchanan, G.N.; Halligan, S.; Bartram, C.I.; Williams, A.B.; Tarroni, D.; Cohen, C.R. Clinical examination, endosonography, and MR imaging in preoperative assessment of fistula in ano: Comparison with outcome-based reference standard. Radiology 2004, 233, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Stevens, T.W.; D’Haens, G.R.; Duijvestein, M.; Bemelman, W.A.; Buskens, C.J.; Gecse, K.B. Diagnostic accuracy of faecal calprotectin in patients with active perianal fistulas. United Eur. Gastroenterol. J. 2019, 7, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Bakan, S.; Olgun, D.C.; Kandemirli, S.G.; Tutar, O.; Samanci, C.; Dikici, S.; Simsek, O.; Rafiee, B.; Adaletli, I.; Mihmanli, I. Perianal Fistula With and Without Abscess: Assessment of Fistula Activity Using Diffusion-Weighted Magnetic Resonance Imaging. Iran J. Radiol 2015, 12, e29084. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Z.; Ouboter, L.F.; Peeters, K.C.M.J.; Hawinkels, L.J.A.C.; Holman, F.; Pascutti, M.F.; Barnhoorn, M.C.; van der Meulen-de Jong, A.E. Crohn’s Disease-Associated and Cryptoglandular Fistulas: Differences and Similarities. J. Clin. Med. 2023, 12, 466. https://doi.org/10.3390/jcm12020466
Zhou Z, Ouboter LF, Peeters KCMJ, Hawinkels LJAC, Holman F, Pascutti MF, Barnhoorn MC, van der Meulen-de Jong AE. Crohn’s Disease-Associated and Cryptoglandular Fistulas: Differences and Similarities. Journal of Clinical Medicine. 2023; 12(2):466. https://doi.org/10.3390/jcm12020466
Chicago/Turabian StyleZhou, Zhou, Laura F. Ouboter, Koen C. M. J. Peeters, Lukas J. A. C. Hawinkels, Fabian Holman, Maria F. Pascutti, Marieke C. Barnhoorn, and Andrea E. van der Meulen-de Jong. 2023. "Crohn’s Disease-Associated and Cryptoglandular Fistulas: Differences and Similarities" Journal of Clinical Medicine 12, no. 2: 466. https://doi.org/10.3390/jcm12020466