Observing an aorto-ostial lesion using TELESCOPE® in optical coherence tomography-guided percutaneous coronary intervention
Supported by the EuroIntervention Journal
Authors
Kazumasa Kurogi1, Masanobu Ishii1, Kenji Sakamoto2, Kenichi Tsujita2
Case summary
We successfully observed an aorto-ostial lesion in optical coherence tomography-guided (OCT) (Abbott Vascular, Santa Clara, CA) percutaneous coronary intervention (PCI) in a 72-year-old female who underwent PCI due to effort angina.
The target lesion was between the left main trunk (LMT) and left anterior descending artery (LAD). After preparing the lesion by balloon angioplasty, a Xience Sierra® everolimus-eluting stent (2.75 x 28 mm and 3.0 x 18 mm; Abbott Vascular, Santa Clare, CA) was implanted from the LAD to LMT ostium (Panel A).

Figure 1. OCT and IVUS findings in aorto-ostial lesion
(A) Final angiography post percutaneous coronary intervention; (B) Optical coherence tomography (OCT) pull-back with Telescope®-guiding extension catheter engaged in left main trunk; (C-G); OCT image from left main trunk to aorta; (C’-G’) Intravascular ultrasound image from left main trunk to aorta; (F, F’) Stent proximal edge level; (F-G) Blood in the aorta; (*) (G, G’) Aorto-ostial junction level
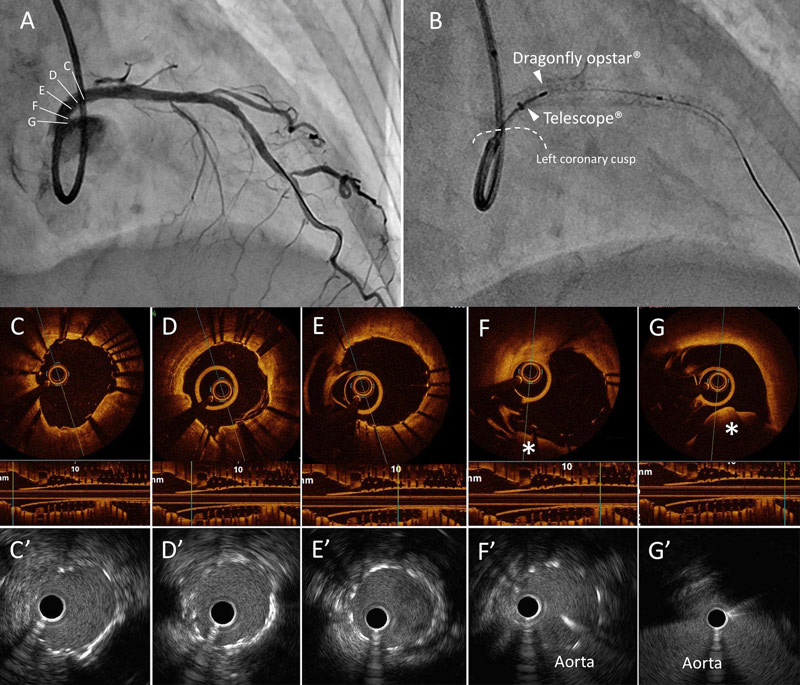
After stent optimization using a 4.0-mm non-compliant balloon, a 6Fr Telescope®-guiding extension catheter (Medtronic Cardiovascular, Santa Rosa, CA) was engaged into the LMT to obtain an OCT image (Panel B). The image showed excellent stent expansion (Panels C-F). Furthermore, the OCT successfully visualized the stent proximal edge near the aorto-ostial lesion through the Telescope®-guiding extension catheter (Panel F-G). An intravascular ultrasound revealed the stent was implanted in the aorto-ostial junction (Panel F’-G’).
Hence, we successfully acquired an OCT image throughout the soft polymer tip and the relatively wide gap of the helical coil reinforcement made from near-infrared transparent material.
The telescope®-guiding extension catheter allows observation of aorto-ostial lesions, which remains a challenge and a significant limitation in OCT-guided PCI.
Conflict of interest statement
Dr. Tsujita has received honoraria from Bayer Yakuhin, Ltd., Daiichi Sankyo Co., Ltd., Kowa Pharmaceutical Co. Ltd., MSD K.K., Sanofi K.K., and Takeda Pharmaceutical Co., Ltd.; trust research/joint research funds from AstraZeneca K.K., Sugi Bee Garden, and Japan Medical Device Technology Co., Ltd.; and scholarship funds from ITI Co., Ltd., Astellas Pharma Inc, Abbott Vascular Japan Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Kaneka Medix Co., Ltd., Goodman Co., Ltd., GM Medical Co., Ltd., Daiichi Sankyo Co., Ltd., Takeda Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma, Chugai Pharmaceutical Co., Ltd., TERUMO Co., Ltd., Boehringer Ingelheim Japan, Medtronic Japan Co., Ltd., Japan Lifeline Co., Ltd., Novartis Pharma K.K., Fides-One, Inc., Bristol-Myers K.K., Boston Scientific Japan K.K., Cardinal Health Japan, and MSD K.K.
Dr. Sakamoto has received trust research/joint research funds from Daiichi Sankyo Co., Ltd.
All the other authors have nothing to disclose.
Affiliations
- Department of Cardiovascular Center, Miyazaki Prefectural Nobeoka Hospital, Nobeoka, Japan
- Department of Cardiovascular Medicine, Graduate School of Medical Sciences, Kumamoto University, Kumamoto, Japan
References
- Maehara A, Matsumura M, Ali ZA, Mintz GS, Stone GW. IVUS-Guided Versus OCT-Guided Coronary Stent Implantation: A Critical Appraisal. J Am Coll Cardiol Img 2017; 10:1487–1503.
No comments yet!