
Albuminuria, Forgotten No More: Underlining the Emerging Role in CardioRenal Crosstalk

 and
and
Abstract
:1. Introduction
2. Conceptual Evolution of Albuminuria as a Cardiac and Renal Biomarker
2.1. Redefining Albuminuria
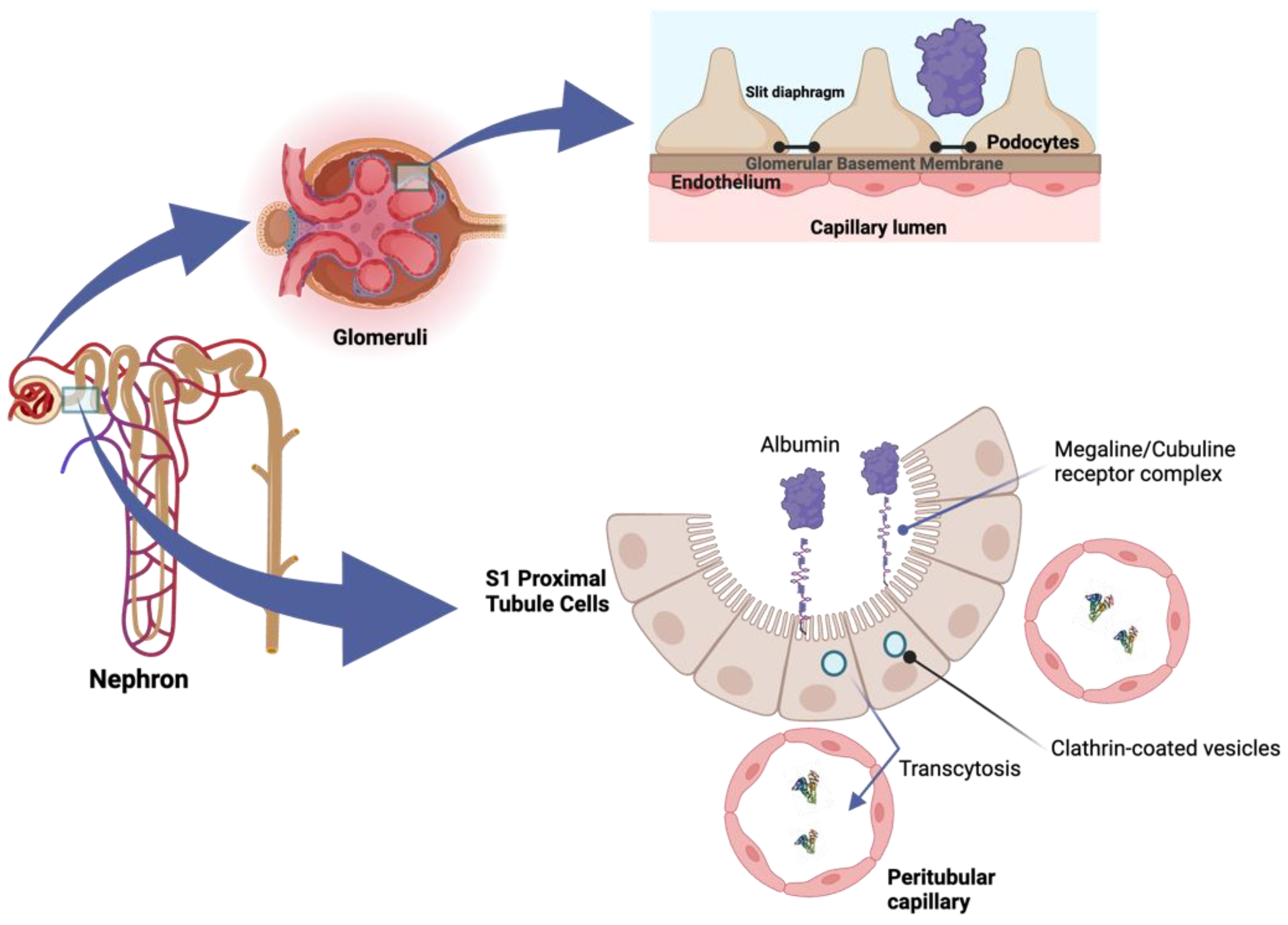
2.2. Understanding the Pathophysiology of Albuminuria
2.3. Albuminuria: The Neglected Biomarker
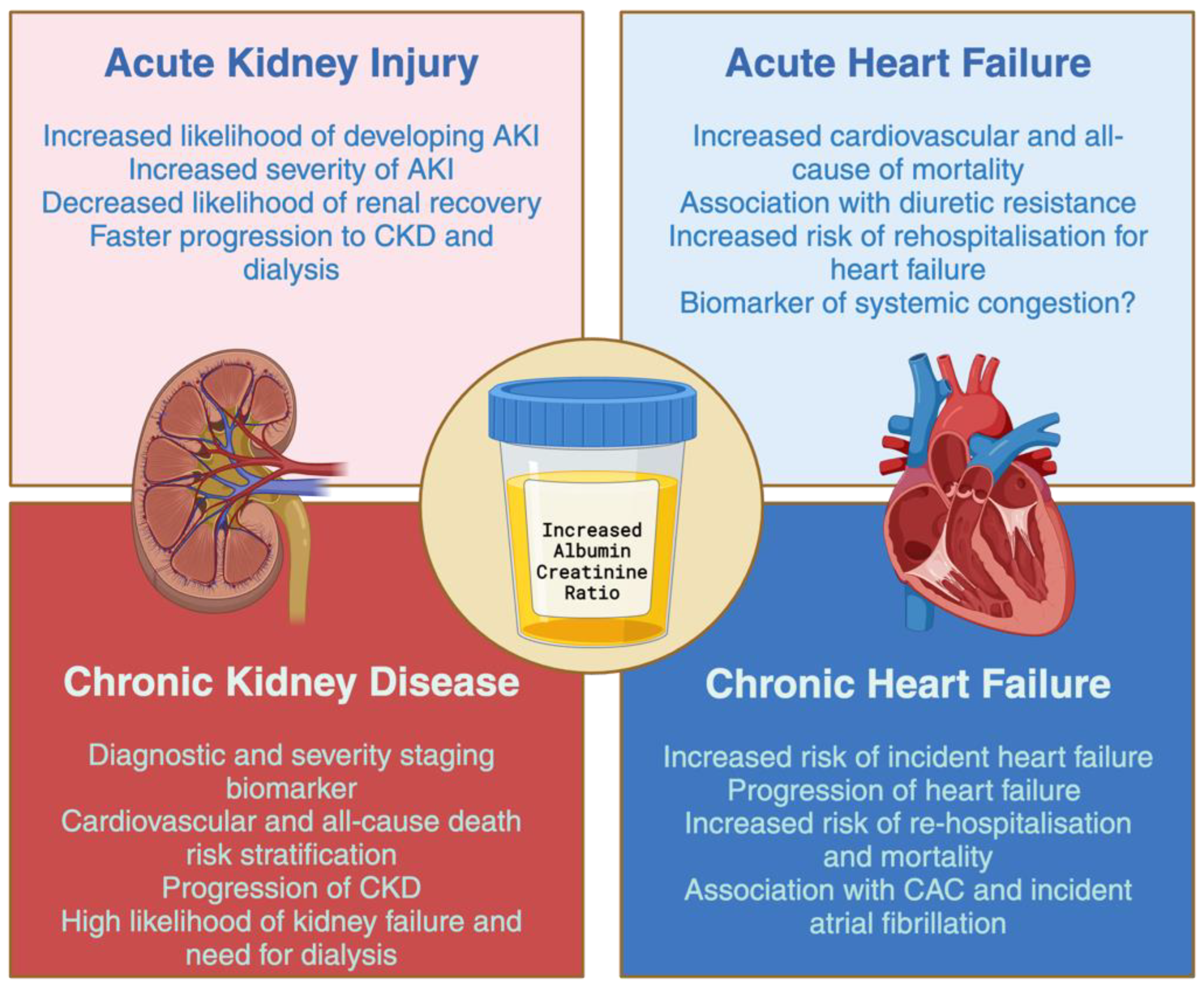
3. Albuminuria in the Continuum of Cardiorenal Disease
3.1. Albuminuria and Acute Kidney Injury
3.2. Albuminuria and Chronic Kidney Disease
3.3. Albuminuria and Congestive Acute Heart Failure
3.4. Albuminuria and Heart Failure
4. Minimizing Albuminuria: Old and New Approaches
4.1. RAS Inhibitors
4.2. Sodium–Glucose Cotrasporter-2 Inhibitors
4.3. Glucagon-Like Peptide 1 Receptor Agonist
4.4. Mineralocorticoid Receptor Antagonist
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levey, A.S.; Grams, M.E.; Inker, L.A. Uses of GFR and Albuminuria Level in Acute and Chronic Kidney Disease. N. Engl. J. Med. 2022, 386, 2120–2128. [Google Scholar] [CrossRef]
- Ronco, C.; Haapio, M.; House, A.A.; Anavekar, N.; Bellomo, R. Cardiorenal Syndrome. J. Am. Coll. Cardiol. 2008, 52, 1527–1539. [Google Scholar] [CrossRef]
- Rangaswami, J.; Bhalla, V.; Blair, J.E.A.; Chang, T.I.; Costa, S.; Lentine, K.L.; Lerma, E.V.; Mezue, K.; Molitch, M.; Mullens, W.; et al. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement from the American Heart Association. Circulation 2019, 139, E840–E878. [Google Scholar] [CrossRef]
- Mullens, W.; Damman, K.; Testani, J.M.; Martens, P.; Mueller, C.; Lassus, J.; Tang, W.H.W.; Skouri, H.; Verbrugge, F.H.; Orso, F.; et al. Evaluation of kidney function throughout the heart failure trajectory—A position statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 584–603. [Google Scholar] [CrossRef]
- Romero-González, G.; González, A.; López, B.; Ravassa, S.; Díez, J. Heart failure in chronic kidney disease: The emerging role of myocardial fibrosis. Nephrol. Dial. Transplant. 2020, 37, 817–824. [Google Scholar] [CrossRef]
- Wang, X.; Shapiro, J.I. Evolving concepts in the pathogenesis of uraemic cardiomyopathy. Nat. Rev. Nephrol. 2019, 15, 159–175. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; Rossignol, P. Cardiorenal syndrome revisited. Circulation 2018, 138, 929–944. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Niño, M.D.; Sanz, A.B.; Ramos, A.M.; Fernandez-Fernandez, B.; Ortiz, A. Clinical proteomics in kidney disease as an exponential technology: Heading towards the disruptive phase. Clin. Kidney J. 2017, 10, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Eckardt, K.U.; Dorman, N.M.; Christiansen, S.L.; Hoorn, E.J.; Ingelfinger, J.R.; Inker, L.A.; Levin, A.; Mehrotra, R.; Palevsky, P.M.; et al. Nomenclature for kidney function and disease: Report of a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Int. 2020, 97, 1117–1129. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.M.; De Jong, P.E.; Griffith, K.E.; et al. Kidney disease: Improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar] [CrossRef]
- Writing Group for the CKD Prognosis Consortium; Appel, L.J.; Grams, M.; Woodward, M.; Harris, K.; Arima, H.; Chalmers, J.; Yatsuya, H.; Tamakoshi, K.; Li, Y.; et al. Estimated Glomerular Filtration Rate, Albuminuria, and Adverse Outcomes: An Individual-Participant Data Meta-Analysis. JAMA 2023, 330, 1266–1277. [Google Scholar] [CrossRef]
- Wong, F. Drug Insight: The role of albumin in the management of chronic liver disease. Nat. Clin. Pract. Gastroenterol. Hepatol. 2007, 4, 43–51. [Google Scholar] [CrossRef]
- Paar, M.; Fengler, V.H.; Rosenberg, D.J.; Krebs, A.; Stauber, R.E.; Oettl, K.; Hammel, M. Albumin in patients with liver disease shows an altered conformation. Commun. Biol. 2021, 4, 731. [Google Scholar] [CrossRef]
- Merlot, A.M.; Kalinowski, D.S.; Richardson, D.R. Unraveling the mysteries of serum albumin-more than just a serum protein. Front. Physiol. 2014, 5, 299. [Google Scholar] [CrossRef] [PubMed]
- Molitoris, B.A.; Sandoval, R.M.; Yadav, S.P.S.; Wagner, M.C. Albumin Uptake and Processing by the Proximal Tubule: Physiological, Pathological, and Therapeutic Implications. Physiol. Rev. 2022, 102, 1625–1667. [Google Scholar] [CrossRef]
- Gupta, R.; Testani, J.; Collins, S. Diuretic Resistance in Heart Failure. Curr. Heart Fail. Rep. 2019, 16, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Shahid, I.; Anker, S.D.; Fonarow, G.C.; Fudim, M.; Hall, M.E.; Hernandez, A.; Morris, A.A.; Shafi, T.; Weir, M.R.; et al. Albuminuria and Heart Failure: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2023, 81, 270–282. [Google Scholar] [CrossRef]
- Devuyst, O.; Ronco, P. Tubular handling of filtered albumin. Kidney Int. 2023, 104, 1073–1075. [Google Scholar] [CrossRef]
- Gburek, J.; Konopska, B.; Gołąb, K. Renal Handling of Albumin—From Early Findings to Current Concepts. Int. J. Mol. Sci. 2021, 22, 5809. [Google Scholar] [CrossRef]
- Pollak, M.R.; Quaggin, S.E.; Hoenig, M.P.; Dworkin, L.D. The Glomerulus: The Sphere of Influence. Clin. J. Am. Soc. Nephrol. 2014, 9, 1461. [Google Scholar] [CrossRef]
- Kopp, J.B.; Anders, H.J.; Susztak, K.; Podestà, M.A.; Remuzzi, G.; Hildebrandt, F.; Romagnani, P. Podocytopathies. Nat. Rev. Dis. Primers 2020, 6, 68. [Google Scholar] [CrossRef] [PubMed]
- Benzing, T.; Salant, D. Insights into Glomerular Filtration and Albuminuria. N. Engl. J. Med. 2021, 384, 1437–1446. [Google Scholar] [CrossRef] [PubMed]
- Comper, W.D.; Vuchkova, J.; McCarthy, K.J. New insights into proteinuria/albuminuria. Front. Physiol. 2022, 13, 991756. [Google Scholar] [CrossRef]
- Cortinovis, M.; Perico, N.; Ruggenenti, P.; Remuzzi, A.; Remuzzi, G. Glomerular hyperfiltration. Nat. Rev. Nephrol. 2022, 18, 435–451. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, N.R.; Masi, S.; Taddei, S. Rethinking albuminuria as a marker to drive treatment in congestive heart failure. Eur. Heart J. 2023, 44, 381–382. [Google Scholar] [CrossRef]
- Kashani, K.; Rosner, M.H.; Ostermann, M. Creatinine: From physiology to clinical application. Eur. J. Intern. Med. 2020, 72, 9–14. [Google Scholar] [CrossRef]
- Ruilope, L.M.; Ortiz, A.; Lucia, A.; Miranda, B.; Alvarez-Llamas, G.; Barderas, M.G.; Volpe, M.; Ruiz-Hurtado, G.; Pitt, B. Prevention of cardiorenal damage: Importance of albuminuria. Eur. Heart J. 2023, 44, 1112–1123. [Google Scholar] [CrossRef]
- Chu, C.D.; Xia, F.; Du, Y.; Singh, R.; Tuot, D.S.; Lamprea-Montealegre, J.A.; Gualtieri, R.; Liao, N.; Kong, S.X.; Williamson, T.; et al. Estimated Prevalence and Testing for Albuminuria in US Adults at Risk for Chronic Kidney Disease. JAMA Netw. Open 2023, 6, e2326230. [Google Scholar] [CrossRef]
- Mahemuti, N.; Zou, J.; Liu, C.; Xiao, Z.; Liang, F.; Yang, X. Urinary Albumin-to-Creatinine Ratio in Normal Range, Cardiovascular Health, and All-Cause Mortality. JAMA Netw. Open 2023, 6, e2348333. [Google Scholar] [CrossRef]
- Visseren, F.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Ortiz, A.; Quiroga, B.; Díez, J.; Escalada San Martín, F.J.; Ramirez, L.; Pérez Maraver, M.; Martínez-Berganza Asensio, M.L.; Arranz Arija, J.Á.; Alvarez-Ossorio Fernández, J.L.; Córdoba, R.; et al. Artículo especial por el Día Mundial del Riñón: Las sociedades científicas españolas ante la guía ESC 2021 de prevención de la enfermedad vascular: Generalizar la medida de la albuminuria para identificar el riesgo vascular y prevenir la enfermedad vascular. Nefrología 2023, 43, 245–250. [Google Scholar] [CrossRef]
- Jose, M.D.; Raj, R.; Jose, K.; Kitsos, A.; Saunder, T.; McKercher, C.; Radford, J. Competing risks of death and kidney failure in a cohort of Australian adults with severe chronic kidney disease. Med. J. Aust. 2022, 216, 140–146. [Google Scholar] [CrossRef]
- Romero-González, G.; Ravassa, S.; González, O.; Lorenzo, I.; Rojas, M.A.; García-Trigo, I.; García-Fernández, N.; Lavilla, J.; Martín, P.L.; López, B.; et al. Burden and challenges of heart failure in patients with chronic kidney disease. A call to action. Nefrología 2020, 40, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Bellomo, R.; Kellum, J.A. Acute kidney injury. Lancet 2019, 394, 1949–1964. [Google Scholar] [CrossRef] [PubMed]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.; Fitzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, S.L.; Chawla, L.S. Renal Angina. Clin. J. Am. Soc. Nephrol. 2010, 5, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Grams, M.E.; Astor, B.C.; Bash, L.D.; Matsushita, K.; Wang, Y.; Coresh, J. Albuminuria and estimated glomerular filtration rate independently associate with acute kidney injury. J. Am. Soc. Nephrol. 2010, 21, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- James, M.T.; Hemmelgarn, B.R.; Wiebe, N.; Pannu, N.; Manns, B.J.; Klarenbach, S.W.; Tonelli, M. Glomerular filtration rate, proteinuria, and the incidence and consequences of acute kidney injury: A cohort study. Lancet 2010, 376, 2096–2103. [Google Scholar] [CrossRef] [PubMed]
- James, M.T.; Grams, M.E.; Woodward, M.; Elley, C.R.; Green, J.A.; Wheeler, D.C.; De Jong, P.; Gansevoort, R.T.; Levey, A.S.; Warnock, D.G.; et al. A meta-analysis of the association of estimated GFR, albuminuria, diabetes mellitus, and hypertension with acute kidney injury. Am. J. Kidney Dis. 2015, 66, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Luo, E.; Yan, G.; Tang, C.; Wang, L.; Zhang, Q.; Gong, J. Microalbuminuria Complicated with Low Estimated Glomerular Filtration Rate: Early Risk Factors for Contrast-Induced Acute Kidney Injury After Coronary Intervention. Med. Sci. Monit. 2022, 28, e935455. [Google Scholar] [CrossRef]
- Sugimoto, K.; Toda, Y.; Iwasaki, T.; Shimizu, K.; Kanazawa, T.; Muto, N.; Kawase, H.; Morimatsu, H.; Morita, K.; Maeshima, Y.; et al. Urinary Albumin Levels Predict Development of Acute Kidney Injury After Pediatric Cardiac Surgery: A Prospective Observational Study. J. Cardiothorac. Vasc. Anesth. 2016, 30, 64–68. [Google Scholar] [CrossRef]
- Coca, S.G.; Jammalamadaka, D.; Sint, K.; Thiessen Philbrook, H.; Shlipak, M.G.; Zappitelli, M.; Devarajan, P.; Hashim, S.; Garg, A.X.; Parikh, C.R. Preoperative proteinuria predicts acute kidney injury in patients undergoing cardiac surgery. J. Thorac. Cardiovasc. Surg. 2012, 143, 495–502. [Google Scholar] [CrossRef]
- Wu, V.C.; Huang, T.M.; Wu, P.C.; Wang, W.J.; Chao, C.T.; Yang, S.Y.; Shiao, C.C.; Hu, F.C.; Lai, C.F.; Lin, Y.F.; et al. Preoperative proteinuria is associated with long-term progression to chronic dialysis and mortality after coronary artery bypass grafting surgery. PLoS ONE 2012, 7, e27687. [Google Scholar] [CrossRef]
- Molnar, A.O.; Parikh, C.R.; Sint, K.; Coca, S.G.; Koyner, J.; Patel, U.D.; Butrymowicz, I.; Shlipak, M.; Garg, A.X. Association of postoperative proteinuria with AKI after cardiac surgery among patients at high risk. Clin. J. Am. Soc. Nephrol. 2012, 7, 1749–1760. [Google Scholar] [CrossRef]
- Wahl, T.S.; Graham, L.A.; Morris, M.S.; Richman, J.S.; Hollis, R.H.; Jones, C.E.; Itani, K.M.; Wagner, T.H.; Mull, H.J.; Whittle, J.C.; et al. Association Between Preoperative Proteinuria and Postoperative Acute Kidney Injury and Readmission. JAMA Surg. 2018, 153, e182009. [Google Scholar] [CrossRef]
- Neyra, J.A.; Manllo, J.; Li, X.; Jacobsen, G.; Yee, J.; Yessayan, L. Association of de novo Dipstick Albuminuria with Severe Acute Kidney Injury in Critically Ill Septic Patients. Nephron Clin. Pract. 2015, 128, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Tziakas, D.; Chalikias, G.; Kareli, D.; Tsigalou, C.; Risgits, A.; Kikas, P.; Makrygiannis, D.; Chatzikyriakou, S.; Kam-pouromiti, G.; Symeonidis, D.; et al. Spot urine albumin to creatinine ratio outperforms novel acute kidney injury biomarkers in patients with acute myocardial infarction. Int. J. Cardiol. 2015, 197, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Neyra, J.A.; Li, X.; Yessayan, L.; Adams-Huet, B.; Yee, J.; Toto, R.D. Dipstick albuminuria and acute kidney injury recovery in critically ill septic patients. Nephrology 2016, 21, 512–518. [Google Scholar] [CrossRef]
- Lee, B.J.; Go, A.S.; Parikh, R.; Leong, T.K.; Tan, T.C.; Walia, S.; Hsu, R.K.; Liu, K.D.; Hsu, C.Y. Pre-admission proteinuria impacts risk of non-recovery after dialysis-requiring acute kidney injury. Kidney Int. 2018, 93, 968. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Yang, X.; Lei, Y.; Zha, Y.; Liu, H.; Ma, C.; Tian, J.; Chen, P.; Yang, T.; Hou, F.F. Urinary biomarkers at the time of AKI diagnosis as predictors of progression of AKI among patients with acute cardiorenal syndrome. Clin. J. Am. Soc. Nephrol. 2016, 11, 1536–1544. [Google Scholar] [CrossRef] [PubMed]
- Koyner, J.L.; Garg, A.X.; Coca, S.G.; Sint, K.; Thiessen-Philbrook, H.; Patel, U.D.; Shlipak, M.G.; Parikh, C.R. Biomarkers predict progression of acute kidney injury after cardiac surgery. J. Am. Soc. Nephrol. 2012, 23, 905–914. [Google Scholar] [CrossRef]
- Remuzzi, G.; Bertani, T. Pathophysiology of Progressive Nephropathies. N. Engl. J. Med. 1998, 339, 1448–1456. [Google Scholar] [CrossRef]
- Swartling, O.; Rydell, H.; Stendahl, M.; Segelmark, M.; Trolle Lagerros, Y.; Evans, M. CKD Progression and Mortality Among Men and Women: A Nationwide Study in Sweden. Am. J. Kidney Dis. 2021, 78, 190–199.e1. [Google Scholar] [CrossRef] [PubMed]
- Fuhrman, D.Y.; Schneider, M.F.; Dell, K.M.; Blydt-Hansen, T.D.; Mak, R.; Saland, J.M.; Furth, S.L.; Warady, B.A.; Moxey-Mims, M.M.; Schwartz, G.J. Albuminuria, proteinuria, and renal disease progression in children with CKD. Clin. J. Am. Soc. Nephrol. 2017, 12, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Hemmelgarn, B.R.; Manns, B.J.; Lloyd, A.; James, M.T.; Klarenbach, S.; Quinn, R.R.; Wiebe, N.; Tonelli, M. Relation between Kidney Function, Proteinuria, and Adverse Outcomes. JAMA 2010, 303, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Zoppini, G.; Targher, G.; Chonchol, M.; Ortalda, V.; Negri, C.; Stoico, V.; Bonora, E. Predictors of estimated GFR decline in patients with type 2 diabetes and preserved kidney function. Clin. J. Am. Soc. Nephrol. 2012, 7, 401–408. [Google Scholar] [CrossRef]
- Tangri, N.; Stevens, L.A.; Griffith, J.; Tighiouart, H.; Djurdjev, O.; Naimark, D.; Levin, A.; Levey, A.S. A Predictive Model for Progression of Chronic Kidney Disease to Kidney Failure. JAMA 2011, 305, 1553–1559. [Google Scholar] [CrossRef]
- The Kidney Failure Risk Equation. Available online: https://kidneyfailurerisk.com/ (accessed on 28 December 2023).
- Tangri, N.; Grams, M.E.; Levey, A.S.; Coresh, J.; Appel, L.J.; Astor, B.C.; Chodick, G.; Collins, A.J.; Djurdjev, O.; Raina Elley, C.; et al. Multinational Assessment of Accuracy of Equations for Predicting Risk of Kidney Failure: A Meta-analysis. JAMA 2016, 315, 164–174. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Greene, T.; Tighiouart, H.; Gansevoort, R.T.; Coresh, J.; Simon, A.L.; Chan, T.M.; Hou, F.F.; Lewis, J.B.; Locatelli, F.; et al. Change in albuminuria as a surrogate endpoint for progression of kidney disease: A meta-analysis of treatment effects in randomised clinical trials. Lancet Diabetes Endocrinol. 2019, 7, 128–139. [Google Scholar] [CrossRef]
- Palmer, B.F.; Biff Palmer, C.F. Change in albuminuria as a surrogate endpoint for cardiovascular and renal outcomes in patients with diabetes. Diabetes Obes. Metab. 2023, 25, 1434–1443. [Google Scholar] [CrossRef]
- Race, G.A.; Scheifley, C.H.; Edwards, J.E. Albuminuria in Congestive Heart Failure. Available online: https://www.ahajournals.org/doi/pdf/10.1161/01.CIR.13.3.329 (accessed on 28 December 2023).
- Albright, R.; Brensilver, J.; Cortell, S. Proteinuria in Congestive Heart Failure. Am. J. Nephrol. 1983, 3, 272–275. [Google Scholar] [CrossRef]
- Mullens, W.; Abrahams, Z.; Francis, G.S.; Sokos, G.; Taylor, D.O.; Starling, R.C.; Young, J.B.; Tang, W.H.W. Importance of Venous Congestion for Worsening of Renal Function in Advanced Decompensated Heart Failure. J. Am. Coll. Cardiol. 2009, 53, 589–596. [Google Scholar] [CrossRef]
- Hanberg, J.S.; Sury, K.; Perry Wilson, F.; Brisco, M.A.; Ahmad, T.; Ter Maaten, J.M.; Samuel Broughton, J.; Assefa, M.; Wilson Tang, W.H.; Parikh, C.R.; et al. Reduced Cardiac Index Is Not the Dominant Driver of Renal Dysfunction in Heart Failure. J. Am. Coll. Cardiol. 2016, 67, 2199–2208. [Google Scholar] [CrossRef] [PubMed]
- Abuelo, J.G. Normotensive Ischemic Acute Renal Failure. N. Engl. J. Med. 2007, 357, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Mullens, W.; Verbrugge, F.H.; Nijst, P.; Tang, W.H.W. Renal sodium avidity in heart failure: From pathophysiology to treatment strategies. Eur. Heart J. 2017, 38, 1872–1882. [Google Scholar] [CrossRef] [PubMed]
- Boorsma, E.M.; ter Maaten, J.M.; Voors, A.A.; van Veldhuisen, D.J. Renal Compression in Heart Failure: The Renal Tamponade Hypothesis. Heart Fail. 2022, 10, 175–183. [Google Scholar] [CrossRef]
- Husain-Syed, F.; Gröne, H.J.; Assmus, B.; Bauer, P.; Gall, H.; Seeger, W.; Ghofrani, A.; Ronco, C.; Birk, H.W. Congestive nephropathy: A neglected entity? Proposal for diagnostic criteria and future perspectives. ESC Heart Fail. 2021, 8, 183–203. [Google Scholar] [CrossRef] [PubMed]
- Boorsma, E.M.; ter Maaten, J.M.; Damman, K.; van Essen, B.J.; Zannad, F.; van Veldhuisen, D.J.; Samani, N.J.; Dickstein, K.; Metra, M.; Filippatos, G.; et al. Albuminuria as a marker of systemic congestion in patients with heart failure. Eur. Heart J. 2023, 44, 368–380. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.W.; Ke, J.F.; Zhang, Z.H.; Lu, J.X.; Li, L.X. Albuminuria but not low eGFR is closely associated with atherosclerosis in patients with type 2 diabetes: An observational study. Diabetol. Metab. Syndr. 2022, 14, 50. [Google Scholar] [CrossRef]
- De Zeeuw, D.; Remuzzi, G.; Parving, H.H.; Keane, W.F.; Zhang, Z.; Shahinfar, S.; Snapinn, S.; Cooper, M.E.; Mitch, W.E.; Brenner, B.M. Albuminuria, a Therapeutic Target for Cardiovascular Protection in Type 2 Diabetic Patients with Nephropathy. Circulation 2004, 110, 921–927. [Google Scholar] [CrossRef]
- Nayor, M.; Larson, M.G.; Wang, N.; Santhanakrishnan, R.; Lee, D.S.; Tsao, C.W.; Cheng, S.; Benjamin, E.J.; Vasan, R.S.; Levy, D.; et al. The association of chronic kidney disease and microalbuminuria with heart failure with preserved vs. reduced ejection fraction. Eur. J. Heart Fail. 2017, 19, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Waheed, S.; Matsushita, K.; Sang, Y.; Hoogeveen, R.; Ballantyne, C.; Coresh, J.; Astor, B.C. Combined Association of Albuminuria and Cystatin C–Based Estimated GFR with Mortality, Coronary Heart Disease, and Heart Failure Outcomes: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Kidney Dis. 2012, 60, 207. [Google Scholar] [CrossRef] [PubMed]
- Capes, S.E.; Gerstein, H.C.; Negassa, A.; Yusuf, S. Enalapril prevents clinical proteinuria in diabetic patients with low ejection fraction. Diabetes Care 2000, 23, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Shuvy, M.; Zwas, D.R.; Lotan, C.; Keren, A.; Gotsman, I. Albuminuria: Associated with Heart Failure Severity and Impaired Clinical Outcomes. Can. J. Cardiol. 2020, 36, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; Mann, J.F.E.; Yi, Q.; Zinman, B.; Dinneen, S.F.; Hoogwerf, B.; Hallé, J.P.; Young, J.; Rashkow, A.; Joyce, C.; et al. Albuminuria and Risk of Cardiovascular Events, Death, and Heart Failure in Diabetic and Nondiabetic Individuals. JAMA 2001, 286, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Song, J.J.; Lee, K.B.; Hyun, Y.Y.; Kim, H. Trace Albumin in the Urine Dipstick Test is Associated with Coronary Artery Calcification in Korean Adults. Nephron 2018, 140, 169–174. [Google Scholar] [CrossRef]
- Åkerblom, A.; Clare, R.M.; Lokhnygina, Y.; Wallentin, L.; Held, C.; Van De Werf, F.; Moliterno, D.J.; Patel, U.D.; Leonardi, S.; Armstrong, P.W.; et al. Albuminuria and cardiovascular events in patients with acute coronary syndromes: Results from the TRACER trial. Am. Heart J. 2016, 178, 1–8. [Google Scholar] [CrossRef]
- Ha, J.T.; Freedman, S.B.; Kelly, D.M.; Neuen, B.L.; Perkovic, V.; Jun, M.; Badve, S.V. Kidney Function, Albuminuria, and Risk of Incident Atrial Fibrillation: A Systematic Review and Meta-Analysis. Am. J. Kidney Dis. 2023, in press. [Google Scholar] [CrossRef]
- Brenner, B.M.; Cooper, M.E.; de Zeeuw, D.; Keane, W.F.; Mitch, W.E.; Parving, H.H.; Remuzzi, G.; Snapinn, S.M.; Zhang, Z.; Shahinfar, S.; et al. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2001, 345, 861–869. [Google Scholar] [CrossRef]
- Lewis, E.J.; Hunsicker, L.G.; Clarke, W.R.; Berl, T.; Pohl, M.A.; Lewis, J.B.; Ritz, E.; Atkins, R.C.; Rohde, R.; Raz, I. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N. Engl. J. Med. 2001, 345, 851–860. [Google Scholar] [CrossRef]
- Parving, H.H.; Lehnert, H.; Bröchner-Mortensen, J.; Gomis, R.; Andersen, S.; Arner, P. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N. Engl. J. Med. 2001, 345, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Disease, K.; Global Outcomes Diabetes Work Group, I.; de Boer, I.H.; Luiza Caramori, M.; Chan, J.C.; Heerspink, H.J.; Hurst, C.; Khunti, K.; Liew, A.; Michos, E.D.; et al. KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2020, 98, S1–S115. [Google Scholar] [CrossRef]
- Cheung, A.K.; Chang, T.I.; Cushman, W.C.; Furth, S.L.; Hou, F.F.; Ix, J.H.; Knoll, G.A.; Muntner, P.; Pecoits-Filho, R.; Sarnak, M.J.; et al. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021, 99, S1–S87. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Baumbach, A.; Böhm, M.; Burri, H.; Čelutkiene, J.; Chioncel, O.; Cleland, J.G.F.; Coats, A.J.S.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failureDeveloped by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Laverman, G.D.; de Zeeuw, D.; Navis, G. Between-patient differences in the renal response to renin-angiotensin system intervention: Clue to optimising renoprotective therapy? J. Renin Angiotensin Aldosterone Syst. 2002, 3, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, D.C.; Toto, R.D.; Stefánsson, B.V.; Jongs, N.; Chertow, G.M.; Greene, T.; Hou, F.F.; McMurray, J.J.V.; Pecoits-Filho, R.; Correa-Rotter, R.; et al. A pre-specified analysis of the DAPA-CKD trial demonstrates the effects of dapagliflozin on major adverse kidney events in patients with IgA nephropathy. Kidney Int. 2021, 100, 215–224. [Google Scholar] [CrossRef]
- Curovic, V.R.; Jongs, N.; Kroonen, M.Y.A.M.; Zobel, E.H.; Hansen, T.W.; Sen, T.; Laverman, G.D.; Kooy, A.; Persson, F.; Rossing, P.; et al. Optimization of Albuminuria-Lowering Treatment in Diabetes by Crossover Rotation to Four Different Drug Classes: A Randomized Crossover Trial. Diabetes Care 2023, 46, 593–601. [Google Scholar] [CrossRef]
- Mogensen, C.E.; Neldam, S.; Tikkanen, I.; Oren, S.; Viskoper, R.; Watts, R.W.; Cooper, M.E. Randomised controlled trial of dual blockade of renin-angiotensin system in patients with hypertension, microalbuminuria, and non-insulin dependent diabetes: The candesartan and lisinopril microalbuminuria (CALM) study. BMJ 2000, 321, 1440–1444. [Google Scholar] [CrossRef]
- Patel, A. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): A randomised controlled trial. Lancet 2007, 370, 829–840. [Google Scholar] [CrossRef]
- Ravid, M.; Lang, R.; Rachmani, R.; Lishner, M. Long-term Renoprotective Effect of Angiotensin-converting Enzyme Inhibition in Non—Insulin-dependent Diabetes Mellitus: A 7-Year Follow-up Study. Arch. Intern. Med. 1996, 156, 286–289. [Google Scholar] [CrossRef]
- Ravid, M.; Savin, H.; Jutrin, I.; Bental, T.; Katz, B.; Lishner, M. Long-term stabilizing effect of angiotensin-converting enzyme inhibition on plasma creatinine and on proteinuria in normotensive type II diabetic patients. Ann. Intern. Med. 1993, 118, 577–581. [Google Scholar] [CrossRef]
- Barnett, A.H.; Bain, S.C.; Bouter, P.; Karlberg, B.; Madsbad, S.; Jervell, J.; Mustonen, J. Angiotensin-receptor blockade versus converting-enzyme inhibition in type 2 diabetes and nephropathy. N. Engl. J. Med. 2004, 351, 1952–1961. [Google Scholar] [CrossRef] [PubMed]
- Bangalore, S.; Fakheri, R.; Toklu, B.; Messerli, F.H. Diabetes mellitus as a compelling indication for use of renin angiotensin system blockers: Systematic review and meta-analysis of randomized trials. BMJ 2016, 352, i438. [Google Scholar] [CrossRef] [PubMed]
- van der Aart-van der Beek, A.B.; de Boer, R.A.; Heerspink, H.J.L. Kidney and heart failure outcomes associated with SGLT2 inhibitor use. Nat. Rev. Nephrol. 2022, 18, 294–306. [Google Scholar] [CrossRef]
- Verma, S.; McMurray, J.J.V. SGLT2 inhibitors and mechanisms of cardiovascular benefit: A state-of-the-art review. Diabetologia 2018, 61, 2108–2117. [Google Scholar] [CrossRef]
- Meraz-Muñoz, A.Y.; Weinstein, J.; Wald, R. eGFR Decline after SGLT2 Inhibitor Initiation: The Tortoise and the Hare Reimagined. Kidney360 2021, 2, 1042–1047. [Google Scholar] [CrossRef]
- Verma, S.; Mcmurray, J.J.V. The Serendipitous Story of SGLT2 Inhibitors in Heart Failure: New Insights from DECLARE-TIMI 58. Circulation 2019, 139, 2537–2541. [Google Scholar] [CrossRef]
- Waijer, S.W.; Xie, D.; Inzucchi, S.E.; Zinman, B.; Koitka-Weber, A.; Mattheus, M.; von Eynatten, M.; Inker, L.A.; Wanner, C.; Heerspink, H.J.L. Short-term changes in albuminuria and risk of cardiovascular and renal outcomes in type 2 diabetes mellitus: A post hoc analysis of the empa-reg outcome trial. J. Am. Heart Assoc. 2020, 9, 16976. [Google Scholar] [CrossRef] [PubMed]
- Jongs, N.; Greene, T.; Chertow, G.M.; McMurray, J.J.V.; Langkilde, A.M.; Correa-Rotter, R.; Rossing, P.; Sjöström, C.D.; Stefansson, B.V.; Toto, R.D.; et al. Effect of dapagliflozin on urinary albumin excretion in patients with chronic kidney disease with and without type 2 diabetes: A prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021, 9, 755–766. [Google Scholar] [CrossRef]
- Oshima, M.; Neuen, B.L.; Li, J.W.; Perkovic, V.; Charytan, D.M.; de Zeeuw, D.; Edwards, R.; Greene, T.; Levin, A.; Mahaffey, K.W.; et al. Early Change in Albuminuria with Canagliflozin Predicts Kidney and Cardiovascular Outcomes: A PostHoc Analysis from the CREDENCE Trial. J. Am. Soc. Nephrol. 2020, 31, 2925–2936. [Google Scholar] [CrossRef]
- Ma, Y.; Lin, C.; Cai, X.; Hu, S.; Zhu, X.; Lv, F.; Yang, W.; Ji, L. Baseline eGFR, albuminuria and renal outcomes in patients with SGLT2 inhibitor treatment: An updated meta-analysis. Acta Diabetol. 2023, 60, 435–445. [Google Scholar] [CrossRef]
- Górriz, J.L.; Soler, M.J.; Navarro-González, J.F.; García-Carro, C.; Puchades, M.J.; D’marco, L.; Castelao, A.M.; Fernández-Fernández, B.; Ortiz, A.; Górriz-Zambrano, C.; et al. GLP-1 Receptor Agonists and Diabetic Kidney Disease: A Call of Attention to Nephrologists. J. Clin. Med. 2020, 9, 947. [Google Scholar] [CrossRef]
- Kawanami, D.; Takashi, Y. GLP-1 Receptor Agonists in Diabetic Kidney Disease: From Clinical Outcomes to Mechanisms. Front. Pharmacol. 2020, 11, 967. [Google Scholar] [CrossRef]
- Yuan, D.; Sharma, H.; Krishnan, A.; Vangaveti, V.N.; Malabu, U.H. Effect of glucagon-like peptide 1 receptor agonists on albuminuria in adult patients with type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Obes. Metab. 2022, 24, 1869–1881. [Google Scholar] [CrossRef]
- Bosch, C.; Carriazo, S.; Soler, M.J.; Ortiz, A.; Fernandez-Fernandez, B. Tirzepatide and prevention of chronic kidney disease. Clin. Kidney J. 2023, 16, 797. [Google Scholar] [CrossRef] [PubMed]
- Karakasis, P.; Patoulias, D.; Fragakis, N.; Klisic, A.; Rizzo, M. Effect of Tirzepatide on Albuminuria Levels and Renal Function in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Multilevel Meta-Analysis. Diabetes Obes. Metab. 2023; early view. [Google Scholar] [CrossRef]
- Agarwal, R.; Kolkhof, P.; Bakris, G.; Bauersachs, J.; Haller, H.; Wada, T.; Zannad, F. Steroidal and non-steroidal mineralocorticoid receptor antagonists in cardiorenal medicine. Eur. Heart J. 2021, 42, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Morales, E.; Millet, V.G.; Rojas-Rivera, J.; Huerta, A.; Gutiérrez, E.; Gutiérrez-Solís, E.; Egido, J.; Praga, M. Renoprotective effects of mineralocorticoid receptor blockers in patients with proteinuric kidney diseases. Nephrol. Dial. Transplant. 2013, 28, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Ando, K.; Ohtsu, H.; Uchida, S.; Kaname, S.; Arakawa, Y.; Fujita, T. Anti-albuminuric effect of the aldosterone blocker eplerenone in non-diabetic hypertensive patients with albuminuria: A double-blind, randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2014, 2, 944–953. [Google Scholar] [CrossRef] [PubMed]
- Romero-González, G.; Bover, J.; Arrieta, J.; Salera, D.; Troya, M.; Graterol, F.; Ureña-Torres, P.; Cozzolino, M.; Di Lullo, L.; Cippà, P.E.; et al. The “FIFTY SHADOWS” of the RALES Trial: Lessons about the Potential Risk of Dietary Potassium Supplementation in Patients with Chronic Kidney Disease. J. Clin. Med. 2022, 11, 3970. [Google Scholar] [CrossRef] [PubMed]
- Pereira, E.; Carrño, A.; Bennouna, M.; Ferreras, I. La sombra del RALES es alargada. Aten. Primaria 2010, 42, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Bärfacker, L.; Kuhl, A.; Hillisch, A.; Grosser, R.; Figueroa-Pérez, S.; Heckroth, H.; Nitsche, A.; Ergüden, J.K.; Gielen-Haertwig, H.; Schlemmer, K.H.; et al. Discovery of BAY 94-8862: A nonsteroidal antagonist of the mineralocorticoid receptor for the treatment of cardiorenal diseases. ChemMedChem 2012, 7, 1385–1403. [Google Scholar] [CrossRef]
- Bakris, G.L.; Agarwal, R.; Chan, J.C.; Cooper, M.E.; Gansevoort, R.T.; Haller, H.; Remuzzi, G.; Rossing, P.; Schmieder, R.E.; Nowack, C.; et al. Effect of Finerenone on Albuminuria in Patients with Diabetic Nephropathy: A Randomized Clinical Trial. JAMA 2015, 314, 884–894. [Google Scholar] [CrossRef]
- Fernández-Fernández, B.; Ortiz Arduán, A. Efecto de la finerenona sobre la albuminuria en pacientes con nefropatía diabética. ¿Grandes esperanzas en tiempos difíciles? Nefrología 2016, 8, 20–25. [Google Scholar]
- Bakris, G.L.; Agarwal, R.; Anker, S.D.; Pitt, B.; Ruilope, L.M.; Rossing, P.; Kolkhof, P.; Nowack, C.; Schloemer, P.; Joseph, A.; et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2020, 383, 2219–2229. [Google Scholar] [CrossRef] [PubMed]
- Pitt, B.; Filippatos, G.; Agarwal, R.; Anker, S.D.; Bakris, G.L.; Rossing, P.; Joseph, A.; Kolkhof, P.; Nowack, C.; Schloemer, P.; et al. Cardiovascular Events with Finerenone in Kidney Disease and Type 2 Diabetes. N. Engl. J. Med. 2021, 385, 2252–2263. [Google Scholar] [CrossRef]
- Agarwal, R.; Tu, W.; Farjat, A.E.; Farag, Y.M.K.; Toto, R.; Kaul, S.; Lawatscheck, R.; Rohwedder, K.; Ruilope, L.M.; Rossing, P.; et al. Impact of Finerenone-Induced Albuminuria Reduction on Chronic Kidney Disease Outcomes in Type 2 Diabetes: A Mediation Analysis. Ann. Intern. Med. 2023, 176, 1606–1616. [Google Scholar] [CrossRef] [PubMed]
- Mårup, F.H.; Thomsen, M.B.; Birn, H. Additive effects of dapagliflozin and finerenone on albuminuria in non-diabetic CKD: An open-label randomized clinical trial. Clin. Kidney J. 2023, 17, sfad249. [Google Scholar] [CrossRef] [PubMed]
- Rossing, P.; Caramori, M.L.; Chan, J.C.N.; Heerspink, H.J.L.; Hurst, C.; Khunti, K.; Liew, A.; Michos, E.D.; Navaneethan, S.D.; Olowu, W.A.; et al. Executive summary of the KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease: An update based on rapidly emerging new evidence. Kidney Int. 2022, 102, 990–999. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Degree of Albuminuria/Proteinuria | Normal to Mildly Increased | Moderately Increased | Severely Increased |
|---|---|---|---|
| Spot ACR | <30 mg/g | 30–299 mg/g | ≥300 mg/g |
| Spot PCR | <150 mg/g | 150–499 mg/g | ≥500 mg/g |
| Urine protein dipstick | Negative to trace | Trace to + | + or greater |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-González, G.; Rodríguez-Chitiva, N.; Cañameras, C.; Paúl-Martínez, J.; Urrutia-Jou, M.; Troya, M.; Soler-Majoral, J.; Graterol Torres, F.; Sánchez-Bayá, M.; Calabia, J.; et al. Albuminuria, Forgotten No More: Underlining the Emerging Role in CardioRenal Crosstalk. J. Clin. Med. 2024, 13, 777. https://doi.org/10.3390/jcm13030777
Romero-González G, Rodríguez-Chitiva N, Cañameras C, Paúl-Martínez J, Urrutia-Jou M, Troya M, Soler-Majoral J, Graterol Torres F, Sánchez-Bayá M, Calabia J, et al. Albuminuria, Forgotten No More: Underlining the Emerging Role in CardioRenal Crosstalk. Journal of Clinical Medicine. 2024; 13(3):777. https://doi.org/10.3390/jcm13030777
Chicago/Turabian StyleRomero-González, Gregorio, Néstor Rodríguez-Chitiva, Carles Cañameras, Javier Paúl-Martínez, Marina Urrutia-Jou, Maribel Troya, Jordi Soler-Majoral, Fredzzia Graterol Torres, Maya Sánchez-Bayá, Jordi Calabia, and et al. 2024. "Albuminuria, Forgotten No More: Underlining the Emerging Role in CardioRenal Crosstalk" Journal of Clinical Medicine 13, no. 3: 777. https://doi.org/10.3390/jcm13030777