
Severe COVID-19: Drugs and Clinical Trials
 , , ,
, , , 
Abstract
:1. Introduction
2. Material and Methods
3. Convalescent Plasma Therapy in COVID-19
Criteria to Consider for CP Therapy
4. Monoclonal Antibodies
4.1. mAbs Targeting SARS-CoV-2 Spike Protein
4.2. Spike Neutralizing nAbs: Casirivimab and Imdevimab
4.3. Sotrovimab
4.4. Regdanvimab
4.5. MW33
4.6. XAV-19
4.7. BRII-196 and BRII-198
4.8. Criteria to Consider for mAbs Therapy
5. Immune Response Regulators
5.1. mAbs Targeting IL-6 and IL-1 Receptor
5.2. Tocilizumab
6. mAbs Directed at Inflammatory Targets
Infliximab
7. Drugs That Target Immunomodulatory Pathways
7.1. Baricitinib
7.2. Tofacitinib
7.3. Ruxolitinib
7.4. Statins
7.5. Anakinra
7.6. Fluvoxamine
7.7. PI3K/Akt/mTOR Pathway Inhibitors
7.8. Novaferon
7.9. Vitamin D
7.10. Criteria to Consider for Immune Regulator Drug Therapy
8. Viral Polymerase Inhibitors
8.1. Remdesivir
8.2. Ribavirin
8.3. Favipiravir
8.4. Molnupiravir
8.5. Sofosbuvir and Daclastivir
8.6. Criteria to Consider for Viral Polymerase Inhibitors
9. Corticosteroids
9.1. Dexamethasone
9.2. Methylprednisolone
9.3. Criteria to Consider for Corticosteroids
10. Protease Inhibitors
10.1. Nirmatrelvir/Ritonavir
10.2. Lopinavir/Ritonavir
10.3. Teicoplanin
10.4. Camostat Mesylate
10.5. Alpha-1-Antitrypsin
10.6. Criteria to Consider for Protease Inhibitors
11. Others
11.1. Heparin
11.2. Colchicine
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berekaa, M.M. Insights into the COVID-19 pandemic: Origin, pathogenesis, diagnosis, and therapeutic interventions. Front. Biosci. 2021, 26, 117–139. [Google Scholar] [CrossRef]
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Lf, A.-M.; Dahal, S.; Kumar, H.; Kv, D. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad. Med. J. 2020, 96, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Shereen, M.A.; Khan, S.; Kazmi, A.; Bashir, N.; Siddique, R. COVID-19 infection: Emergence, transmission, and characteristics of human coronaviruses. J. Adv. Res. 2020, 24, 91–98. [Google Scholar] [CrossRef]
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 8 June 2020).
- Number of COVID-19 Patients in ICU per Million. Available online: https://ourworldindata.org/grapher/covid-icu-patients-per-million (accessed on 29 March 2023).
- Tay, M.Z.; Poh, C.M.; Rénia, L.; Macary, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Nile, S.H.; Nile, A.; Qiu, J.; Li, L.; Jia, X.; Kai, G. COVID-19: Pathogenesis, cytokine storm and therapeutic potential of interferons. Cytokine Growth Factor Rev. 2020, 53, 66–70. [Google Scholar] [CrossRef]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef]
- Pijls, B.G.; Jolani, S.; Atherley, A.; Derckx, R.T.; Dijkstra, J.I.R.; Franssen, G.H.L.; Hendriks, S.; Richters, A.; Venemans-Jellema, A.; Zalpuri, S.; et al. Demographic risk factors for COVID-19 infection, severity, ICU admission and death: A meta-analysis of 59 studies. BMJ Open 2021, 11, e044640. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef]
- Zhang, J.-J.; Dong, X.; Liu, G.-H.; Gao, Y.-D. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2022, 64, 90–107. [Google Scholar] [CrossRef]
- Artese, A.; Svicher, V.; Costa, G.; Salpini, R.; Di Maio, V.C.; Alkhatib, M.; Ambrosio, F.A.; Santoro, M.M.; Assaraf, Y.G.; Alcaro, S.; et al. Current status of antivirals and druggable targets of SARS-CoV-2 and other human pathogenic coronaviruses. Drug Resist. Updat. 2020, 53, 100721. [Google Scholar] [CrossRef]
- Kausar, S.; Khan, F.S.; Rehman, M.I.M.U.; Akram, M.; Riaz, M.; Rasool, G.; Khan, A.H.; Saleem, I.; Shamim, S.; Malik, A. A review: Mechanism of action of antiviral drugs. Int. J. Immunopathol. Pharmacol. 2021, 35, 20587384211002621. [Google Scholar] [CrossRef] [PubMed]
- Amin, S.A.; Banerjee, S.; Gayen, S.; Jha, T. Protease targeted COVID-19 drug discovery: What we have learned from the past SARS-CoV inhibitors? Eur. J. Med. Chem. 2021, 215, 113294. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Perera, L.; Tillekeratne, L.V. Potential SARS-CoV-2 main protease inhibitors. Drug Discov. Today 2020, 26, 804–816. [Google Scholar] [CrossRef] [PubMed]
- Batiha, G.E.-S.; Al-Gareeb, A.I.; Saad, H.M.; Al-Kuraishy, H.M. COVID-19 and corticosteroids: A narrative review. Inflammopharmacology 2022, 30, 1189–1205. [Google Scholar] [CrossRef] [PubMed]
- Akter, F.; Araf, Y.; Hosen, M.J. Corticosteroids for COVID-19: Worth it or not? Mol. Biol. Rep. 2021, 49, 567–576. [Google Scholar] [CrossRef]
- Zhang, Y.; Hao, X.; Ma, J.; Wang, M.; Li, Y.; Liu, Y.; Zhao, D.; Zhang, W.; Li, C.; Yan, L.; et al. Phase 1 Safety and Pharmaco-kinetics Studies of BRII-196 and BRII-198, SARS-CoV-2 Spike-Targeting Monoclonal Antibodies. medRxiv 2021. [Google Scholar] [CrossRef]
- Nelson, G.; Buzko, O.; Spilman, P.; Niazi, K.; Rabizadeh, S.; Soon-Shiong, P. Molecular dynamic simulation reveals E484K mutation enhances spike RBD-ACE2 affinity and the combination of E484K, K417N and N501Y mutations (501Y.V2 variant) induces conformational change greater than N501Y mutant alone, potentially resulting in an escape mutant. bioRxiv 2021. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, Y.; Qiao, W.; Zhang, J.; Qi, Z. Baricitinib, a drug with potential effect to prevent SARS-CoV-2 from entering target cells and control cytokine storm induced by COVID-19. Int. Immunopharmacol. 2020, 86, 106749. [Google Scholar] [CrossRef]
- Marrero, M.B. Introduction to JAK/STAT signaling and the vasculature. Vasc. Pharmacol. 2005, 43, 307–309. [Google Scholar] [CrossRef]
- Ko, J.-H.; Seok, H.; Cho, S.Y.; Ha, Y.E.; Baek, J.Y.; Kim, S.H.; Kim, Y.-J.; Park, J.K.; Chung, C.R.; Kang, E.-S.; et al. Challenges of Convalescent Plasma Infusion Therapy in Middle East Respiratory Coronavirus Infection: A Single Centre Experience. Antivir. Ther. 2018, 23, 617–622. [Google Scholar] [CrossRef]
- Hung, I.F.N.; To, K.; Lee, C.-K.; Lee, K.-L.; Chan, K.K.C.; Yan, W.-W.; Liu, R.; Watt, C.-L.; Chan, W.-M.; Lai, K.-Y.; et al. Convalescent Plasma Treatment Reduced Mortality in Patients With Severe Pandemic Influenza A (H1N1) 2009 Virus Infection. Clin. Infect. Dis. 2011, 52, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Zhong, N.; Guan, Y. Treatment with Convalescent Plasma for Influenza A (H5N1) Infection. N. Engl. J. Med. 2007, 357, 1450–1451. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Wong, R.; Soo, Y.O.Y.; Wong, W.S.; Lee, C.K.; Ng, M.H.L.; Chan, P.; Wong, K.C.; Leung, C.B.; Cheng, G. Use of convalescent plasma therapy in SARS patients in Hong Kong. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 24, 44–46. [Google Scholar] [CrossRef] [PubMed]
- Duan, K.; Liu, B.; Li, C.; Zhang, H.; Yu, T.; Qu, J.; Zhou, M.; Chen, L.; Meng, S.; Hu, Y.; et al. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc. Natl. Acad. Sci. USA 2020, 117, 9490–9496. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Wright, R.S.; Fairweather, D.; Senefeld, J.W.; Bruno, K.A.; Klassen, S.A.; Carter, R.E.; Klompas, A.M.; Wiggins, C.C.; Shepherd, J.R.; et al. Early safety indicators of COVID-19 convalescent plasma in 5000 patients. J. Clin. Investig. 2020, 130, 4791–4797. [Google Scholar] [CrossRef]
- Salazar, E.; Christensen, P.A.; Graviss, E.A.; Nguyen, D.T.; Castillo, B.; Chen, J.; Lopez, B.V.; Eagar, T.N.; Yi, X.; Zhao, P.; et al. Treatment of Coronavirus Disease 2019 Patients with Convalescent Plasma Reveals a Signal of Significantly Decreased Mortality. Am. J. Pathol. 2020, 190, 2290–2303. [Google Scholar] [CrossRef]
- Salazar, E.; Perez, K.K.; Ashraf, M.; Chen, J.; Castillo, B.; Christensen, P.A.; Eubank, T.; Bernard, D.W.; Eagar, T.N.; Long, S.W.; et al. Treatment of COVID-19 Patients with Convalescent Plasma in Houston, Texas. medRxiv 2020. [Google Scholar] [CrossRef]
- Bégin, P.; Callum, J.; Jamula, E.; Cook, R.; Heddle, N.M.; Tinmouth, A.; Zeller, M.P.; Beaudoin-Bussières, G.; Amorim, L.; Bazin, R.; et al. Convalescent plasma for hospitalized patients with COVID-19: An open-label, randomized controlled trial. Nat. Med. 2021, 27, 2012–2024. [Google Scholar] [CrossRef]
- Tomaras, G.D.; Ferrari, G.; Shen, X.; Alam, S.M.; Liao, H.-X.; Pollara, J.; Bonsignori, M.; Moody, M.A.; Fong, Y.; Chen, X.; et al. Vaccine-induced plasma IgA specific for the C1 region of the HIV-1 envelope blocks binding and effector function of IgG. Proc. Natl. Acad. Sci. USA 2013, 110, 9019–9024. [Google Scholar] [CrossRef]
- Haynes, B.F.; Gilbert, P.B.; McElrath, M.J.; Zolla-Pazner, S.; Tomaras, G.D.; Alam, S.M.; Evans, D.T.; Montefiori, D.C.; Karnasuta, C.; Sutthent, R.; et al. Immune-Correlates Analysis of an HIV-1 Vaccine Efficacy Trial. N. Engl. J. Med. 2012, 366, 1275–1286. [Google Scholar] [CrossRef]
- Shenoy, A.G.; Hettinger, A.Z.; Fernandez, S.J.; Blumenthal, J.; Baez, V. Early mortality benefit with COVID-19 convalescent plasma: A matched control study. Br. J. Haematol. 2021, 192, 706–713. [Google Scholar] [CrossRef]
- Vlaar, A.P.; Toy, P.; Fung, M.; Looney, M.R.; Juffermans, N.P.; Bux, J.; Bolton-Maggs, P.; Peters, A.L.; Silliman, C.C.; Kor, D.J.; et al. A consensus redefinition of transfusion-related acute lung injury. Transfusion 2019, 59, 2465–2476. [Google Scholar] [CrossRef] [PubMed]
- Gajic, O.; Rana, R.; Winters, J.L.; Yilmaz, M.; Mendez, J.L.; Rickman, O.B.; O’Byrne, M.M.; Evenson, L.K.; Malinchoc, M.; DeGoey, S.R.; et al. Transfusion-related Acute Lung Injury in the Critically Ill. Am. J. Respir. Crit. Care Med. 2012, 176, 886–891. [Google Scholar] [CrossRef] [PubMed]
- Vlaar, A.P.J.; Binnekade, J.M.; Prins, D.; van Stein, D.; Hofstra, J.J.; Schultz, M.J.; Juffermans, N.P. Risk factors and outcome of transfusion-related acute lung injury in the critically ill: A nested case–control study. Crit. Care Med. 2010, 38, 771–778. [Google Scholar] [CrossRef] [PubMed]
- de Alwis, R.; Chen, S.; Gan, E.S.; Ooi, E.E. Impact of immune enhancement on COVID-19 polyclonal hyperimmune globulin therapy and vaccine development. Ebiomedicine 2020, 55, 102768. [Google Scholar] [CrossRef]
- Lutz, H.U. How Immune Complexes from Certain IgG NAbs and Any F(ab′)2 Can Mediate Excessive Complement Activation. Adv. Exp. Med. Biol. 2012, 750, 186–196. [Google Scholar] [CrossRef]
- Kam, Y.W.; Kien, F.; Roberts, A.; Cheung, Y.C.; Lamirande, E.W.; Vogel, L.; Chu, S.L.; Tse, J.; Guarner, J.; Zaki, S.R.; et al. Antibodies against trimeric S glycoprotein protect hamsters against SARS-CoV challenge despite their capacity to mediate FcγRII-dependent entry into B cells in vitro. Vaccine 2007, 25, 729–740. [Google Scholar] [CrossRef]
- Acosta-Ampudia, Y.; Monsalve, D.M.; Rojas, M.; Rodríguez, Y.; Gallo, J.E.; Salazar-Uribe, J.C.; Santander, M.J.; Cala, M.P.; Zapata, W.; Zapata, M.I.; et al. COVID-19 convalescent plasma composition and immunological effects in severe patients. J. Autoimmun. 2021, 118, 102598. [Google Scholar] [CrossRef]
- Iannizzi, C.; Chai, K.L.; Piechotta, V.; Valk, S.J.; Kimber, C.; Monsef, I.; Wood, E.M.; A Lamikanra, A.; Roberts, D.J.; McQuilten, Z.; et al. Convalescent plasma for people with COVID-19: A living systematic review. Cochrane Database Syst. Rev. 2023, 2, CD013600. [Google Scholar] [CrossRef]
- Rojas, M.; Anaya, J.-M. Why will it never be known if convalescent plasma is effective for COVID-19. J. Transl. Autoimmun. 2020, 3, 100069. [Google Scholar] [CrossRef]
- Bloch, E.M.; Shoham, S.; Casadevall, A.; Sachais, B.S.; Shaz, B.; Winters, J.L.; Van Buskirk, C.; Grossman, B.J.; Joyner, M.; Henderson, J.P.; et al. Deployment of convalescent plasma for the prevention and treatment of COVID-19. J. Clin. Investig. 2020, 130, 2757–2765. [Google Scholar] [CrossRef] [PubMed]
- Busch, M.P.; Bloch, E.M.; Kleinman, S.H. Prevention of transfusion-transmitted infections. Blood 2019, 133, 1854–1864. [Google Scholar] [CrossRef] [PubMed]
- Hendrickson, J.E.; Hillyer, C.D. Noninfectious Serious Hazards of Transfusion. Obstet. Anesth. Dig. 2009, 108, 759–769. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Shang, J.; Sun, S.; Tai, W.; Chen, J.; Geng, Q.; He, L.; Chen, Y.; Wu, J.; Shi, Z.; et al. Molecular Mechanism for Antibody-Dependent Enhancement of Coronavirus Entry. J. Virol. 2020, 94, e02015–e02019. [Google Scholar] [CrossRef] [PubMed]
- Tetro, J.A. Is COVID-19 receiving ADE from other coronaviruses? Microbes Infect. 2020, 22, 72–73. [Google Scholar] [CrossRef]
- Bosboom, J.J.; Klanderman, R.B.; Migdady, Y.; Bolhuis, B.; Veelo, D.P.; Geerts, B.F.; Murphy, M.F.; Vlaar, A.P. Transfusion-Associated Circulatory Overload: A Clinical Perspective. Transfus. Med. Rev. 2019, 33, 69–77. [Google Scholar] [CrossRef]
- Agnihotri, N.; Agnihotri, A. Transfusion associated circulatory overload. Indian J. Crit. Care Med. 2014, 18, 396–398. [Google Scholar] [CrossRef]
- Toy, P.; Lowell, C. TRALI—Definition, mechanisms, incidence and clinical relevance. Best Pract. Res. Clin. Anaesthesiol. 2007, 21, 183–193. [Google Scholar] [CrossRef]
- Roubinian, N. TACO and TRALI: Biology, risk factors, and prevention strategies. Hematology 2018, 2018, 585–594. [Google Scholar] [CrossRef]
- D’Souza, R.; Ashraf, R.; Rowe, H.; Zipursky, J.; Clarfield, L.; Maxwell, C.; Arzola, C.; Lapinsky, S.; Paquette, K.; Murthy, S.; et al. Pregnancy and COVID -19: Pharmacologic considerations. Ultrasound Obstet. Gynecol. 2020, 57, 195–203. [Google Scholar] [CrossRef]
- Sajmi, S.; Goutham, K.; Arumugam, V.; Gopalakrishnan, N.; Lamech, T.M.; Aiswarya, D.; Krishna, R.; Vathsalyan, P.; Kannan, B.S.; Solomon, D.; et al. Efficacy and safety of convalescent plasma therapy in SARS-CoV2 patients on hemodialysis. Hemodial. Int. 2021, 25, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Xiao, J.; Hooper, A.T.; Hamilton, J.D.; Musser, B.J.; et al. REGEN-COV Antibody Combination and Outcomes in Outpatients with COVID-19. N. Engl. J. Med. 2021, 385, e81. [Google Scholar] [CrossRef] [PubMed]
- Dougan, M.; Nirula, A.; Azizad, M.; Mocherla, B.; Gottlieb, R.L.; Chen, P.; Hebert, C.; Perry, R.; Boscia, J.; Heller, B.; et al. Bamlanivimab plus Etesevimab in Mild or Moderate COVID-19. N. Engl. J. Med. 2021, 385, 1382–1392. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gonzalez-Rojas, Y.; Juarez, E.; Casal, M.C.; Moya, J.; Falci, D.R.; Sarkis, E.; Solis, J.; Zheng, H.; Scott, N.; et al. Early Treatment for COVID-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N. Engl. J. Med. 2021, 385, 1941–1950. [Google Scholar] [CrossRef]
- A Neutralizing Monoclonal Antibody for Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 905–914. [CrossRef] [PubMed]
- Nishimoto, N.; Kishimoto, T. Humanized Antihuman IL-6 Receptor Antibody, Tocilizumab. Handb. Exp. Pharmacol. 2008, 181, 151–160. [Google Scholar] [CrossRef]
- Tuccori, M.; Ferraro, S.; Convertino, I.; Cappello, E.; Valdiserra, G.; Blandizzi, C.; Maggi, F.; Focosi, D. Anti-SARS-CoV-2 neutralizing monoclonal antibodies: Clinical pipeline. Mabs 2020, 12, 1854149. [Google Scholar] [CrossRef]
- Jaworski, J.P. Neutralizing monoclonal antibodies for COVID-19 treatment and prevention. Biomed. J. 2020, 44, 7–17. [Google Scholar] [CrossRef]
- Sui, J.; Li, W.; Murakami, A.; Tamin, A.; Matthews, L.J.; Wong, S.K.; Moore, M.J.; Tallarico, A.S.C.; Olurinde, M.; Choe, H.; et al. Potent neutralization of severe acute respiratory syndrome (SARS) coronavirus by a human mAb to S1 protein that blocks receptor association. Proc. Natl. Acad. Sci. USA 2004, 101, 2536–2541. [Google Scholar] [CrossRef]
- Elshabrawy, H.A.; Coughlin, M.M.; Baker, S.C.; Prabhakar, B.S. Human Monoclonal Antibodies against Highly Conserved HR1 and HR2 Domains of the SARS-CoV Spike Protein Are More Broadly Neutralizing. PLoS ONE 2012, 7, e50366. [Google Scholar] [CrossRef]
- Zhu, Z.; Chakraborti, S.; He, Y.; Roberts, A.; Sheahan, T.; Xiao, X.; Hensley, L.E.; Prabakaran, P.; Rockx, B.; Sidorov, I.A.; et al. Potent cross-reactive neutralization of SARS coronavirus isolates by human monoclonal antibodies. Proc. Natl. Acad. Sci. USA 2007, 104, 12123–12128. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, M.M.; Prabhakar, B.S. Neutralizing human monoclonal antibodies to severe acute respiratory syndrome coronavirus: Target, mechanism of action, and therapeutic potential. Rev. Med. Virol. 2011, 22, 2–17. [Google Scholar] [CrossRef] [PubMed]
- Van Erp, E.A.; Luytjes, W.; Ferwerda, G.; Van Kasteren, P.B. Fc-Mediated Antibody Effector Functions During Respiratory Syncytial Virus Infection and Disease. Front. Immunol. 2019, 10, 548. [Google Scholar] [CrossRef] [PubMed]
- Beebe, D.P.; Cooper, N.R. Neutralization of vesicular stomatitis virus (VSV) by human complement requires a natural IgM antibody present in human serum. J. Immunol. 1981, 126, 1562–1568. [Google Scholar] [CrossRef]
- Liu, H.; Wei, P.; Zhang, Q.; Chen, Z.; Aviszus, K.; Downing, W.; Peterson, S.; Reynoso, L.; Downey, G.P.; Frankel, S.K.; et al. 501Y.V2 and 501Y.V3 Variants of SARS-CoV-2 Lose Binding to Bamlanivimab in Vitro. bioRxiv 2021. [Google Scholar] [CrossRef]
- Wu, K.; Werner, A.P.; Koch, M.; Choi, A.; Narayanan, E.; Stewart-Jones, G.B.; Colpitts, T.; Bennett, H.; Boyoglu-Barnum, S.; Shi, W.; et al. Serum Neutralizing Activity Elicited by mRNA-1273 Vaccine. N. Engl. J. Med. 2021, 384, 1468–1470. [Google Scholar] [CrossRef]
- Chen, X.; Li, R.; Pan, Z.; Qian, C.; Yang, Y.; You, R.; Zhao, J.; Liu, P.; Gao, L.; Li, Z.; et al. Human monoclonal antibodies block the binding of SARS-CoV-2 spike protein to angiotensin converting enzyme 2 receptor. Cell Mol. Immunol. 2020, 17, 647–649. [Google Scholar] [CrossRef]
- Ju, B.; Zhang, Q.; Ge, J.; Wang, R.; Sun, J.; Ge, X.; Yu, J.; Shan, S.; Zhou, B.; Song, S.; et al. Human neutralizing antibodies elicited by SARS-CoV-2 infection. Nature 2020, 584, 115–119. [Google Scholar] [CrossRef]
- Rogers, T.F.; Zhao, F.; Huang, D.; Beutler, N.; Burns, A.; He, W.-T.; Limbo, O.; Smith, C.; Song, G.; Woehl, J.; et al. Isolation of potent SARS-CoV-2 neutralizing antibodies and protection from disease in a small animal model. Science 2020, 369, 956–963. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, F.; Shen, C.; Peng, W.; Li, D.; Zhao, C.; Li, Z.; Li, S.; Bi, Y.; Yang, Y.; et al. A noncompeting pair of human neutralizing antibodies block COVID-19 virus binding to its receptor ACE2. Science 2020, 368, 1274–1278. [Google Scholar] [CrossRef]
- Wang, S.; Peng, Y.; Wang, R.; Jiao, S.; Wang, M.; Huang, W.; Shan, C.; Jiang, W.; Li, Z.; Gu, C.; et al. Characterization of neutralizing antibody with prophylactic and therapeutic efficacy against SARS-CoV-2 in rhesus monkeys. Nat. Commun. 2020, 11, 5752. [Google Scholar] [CrossRef] [PubMed]
- Somersan-Karakaya, S.; Mylonakis, E.; Menon, V.P.; Wells, J.C.; Ali, S.; Sivapalasingam, S.; Sun, Y.; Bhore, R.; Mei, J.; Miller, J.; et al. Casirivimab and Imdevimab for the Treatment of Hospitalized Patients With COVID-19. J. Infect. Dis. 2022, 227, 23–34. [Google Scholar] [CrossRef] [PubMed]
- O’brien, M.P.; Forleo-Neto, E.; Musser, B.J.; Isa, F.; Chan, K.-C.; Sarkar, N.; Bar, K.J.; Barnabas, R.V.; Barouch, D.H.; Cohen, M.S.; et al. Subcutaneous REGEN-COV Antibody Combination to Prevent COVID-19. N. Engl. J. Med. 2021, 385, 1184–1195. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Wang, P.; Xiong, Y.; Wu, Y.; Lin, X.; Lu, S.; Li, R.; Zhao, B.; Liu, J.; Zeng, S.; et al. Safety, Tolerability, Pharmacokinetic Characteristics, and Immunogenicity of MW33: A Phase 1 Clinical Study of the SARS-CoV-2 RBD-Targeting Monoclonal Antibody Tolerability, Pharmacokinetic Characteristics, and Immunogenicity of MW33: A Phase 1 Clinical Study of the SARS-CoV-2 RBD-Targeting Monoclonal Antibody. Emerg. Microbes Infect. 2021, 10, 1638–1648. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Sandkovsky, U.; Reilly, C.S.; Vock, D.M.; Gottlieb, R.L.; Mack, M.; Golden, K.; Dishner, E.; Vekstein, A.; Ko, E.R.; et al. Efficacy and safety of two neutralising monoclonal antibody therapies, sotrovimab and BRII-196 plus BRII-198, for adults hospitalised with COVID-19 (TICO): A randomised controlled trial. Lancet Infect. Dis. 2022, 22, 622–635. [Google Scholar] [CrossRef]
- Rose, M.; Guy, L.; Shamblen, S.; Guest, G.; Gilbertson, A.; Peiper, N. LB11. Preliminary Findings from a HIV Self-Testing Program among People Who Use Drugs. Open Forum Infect. Dis. 2021, 8, S810–S811. [Google Scholar] [CrossRef]
- Vanhove, B.; Marot, S.; So, R.T.; Gaborit, B.; Evanno, G.; Malet, I.; Lafrogne, G.; Mevel, E.; Ciron, C.; Royer, P.J.; et al. XAV-19, a Swine Glyco-Humanized Polyclonal Antibody Against SARS-CoV-2 Spike Receptor-Binding Domain, Targets Multiple Epitopes and Broadly Neutralizes Variants. Front. Immunol. 2021, 12, 4597. [Google Scholar] [CrossRef]
- Heo, Y.A. Sotrovimab: First Approval. Drugs 2022, 82, 477–484. [Google Scholar] [CrossRef]
- Maher, M.C.; Soriaga, L.B.; Gupta, A.; Chen, Y.-P.; di Iulio, J.; Ledoux, S.; Smithey, M.J.; Cathcart, A.L.; McKusick, K.; Sun, D.; et al. Antibody therapy reverses biological signatures of COVID-19 progression. Cell Rep. Med. 2022, 3, 100721. [Google Scholar] [CrossRef]
- Kim, J.Y.; Jang, Y.R.; Hong, J.H.; Jung, J.G.; Park, J.-H.; Streinu-Cercel, A.; Streinu-Cercel, A.; Săndulescu, O.; Lee, S.J.; Kim, S.H.; et al. Safety, Virologic Efficacy, and Pharmacokinetics of CT-P59, a Neutralizing Monoclonal Antibody Against SARS-CoV-2 Spike Receptor-Binding Protein: Two Randomized, Placebo-Controlled, Phase I Studies in Healthy Individuals and Patients With Mild SARS-CoV-2 Infection. Clin. Ther. 2021, 43, 1706–1727. [Google Scholar] [CrossRef]
- Dumet, C.; Jullian, Y.; Musnier, A.; Rivière, P.; Poirier, N.; Watier, H.; Bourquard, T.; Poupon, A. Exploring Epitope and Functional Diversity of Anti-SARS-CoV2 Antibodies Using AI-Based Methods. bioRxiv 2020. [Google Scholar] [CrossRef]
- Deeks, E.D. Casirivimab/Imdevimab: First Approval. Drugs 2021, 81, 2047–2055. [Google Scholar] [CrossRef] [PubMed]
- Pallotta, A.M.; Kim, C.; Gordon, S.M.; Kim, A. Monoclonal antibodies for treating COVID-19. Clevel. Clin. J. Med. 2021. [Google Scholar] [CrossRef]
- Ozono, S.; Zhang, Y.; Ode, H.; Sano, K.; Tan, T.S.; Imai, K.; Miyoshi, K.; Kishigami, S.; Ueno, T.; Iwatani, Y.; et al. SARS-CoV-2 D614G spike mutation increases entry efficiency with enhanced ACE2-binding affinity. Nat. Commun. 2021, 12, 848. [Google Scholar] [CrossRef] [PubMed]
- Greaney, A.J.; Loes, A.N.; Crawford, K.H.; Starr, T.N.; Malone, K.D.; Chu, H.Y.; Bloom, J.D. Comprehensive mapping of mutations in the SARS-CoV-2 receptor-binding domain that affect recognition by polyclonal human plasma antibodies. Cell Host Microbe 2021, 29, 463–476.e6. [Google Scholar] [CrossRef]
- Weisblum, Y.; Schmidt, F.; Zhang, F.; DaSilva, J.; Poston, D.; Lorenzi, J.C.; Muecksch, F.; Rutkowska, M.; Hoffmann, H.-H.; Michailidis, E.; et al. Escape from neutralizing antibodies by SARS-CoV-2 spike protein variants. eLife 2020, 9, e61312. [Google Scholar] [CrossRef]
- Tada, T.; Dcosta, B.M.; Zhou, H.; Vaill, A.; Kazmierski, W.; Landau, N.R. Decreased Neutralization of SARS-CoV-2 Global Variants by Therapeutic Anti-Spike Protein Monoclonal Antibodies. bioRxiv 2021. [Google Scholar] [CrossRef]
- Zhou, H.; Dcosta, B.M.; Samanovic, M.I.; Mulligan, M.J.; Landau, N.R.; Tada, T.B. 1.526 SARS-CoV-2 Variants Identified in New York City Are Neutralized by Vaccine-Elicited and Therapeutic Monoclonal Antibodies. mBio 2021, 12, 4. [Google Scholar] [CrossRef]
- Kreuzberger, N.; Hirsch, C.; Chai, K.L.; Piechotta, V.; Valk, S.J.; Estcourt, L.J.; Salomon, S.; Tomlinson, E.; Monsef, I.; Wood, E.M.; et al. SARS-CoV-2-neutralising monoclonal antibodies for treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 1, CD013825. [Google Scholar] [CrossRef]
- Wang, P.; Nair, M.S.; Liu, L.; Iketani, S.; Luo, Y.; Guo, Y.; Wang, M.; Yu, J.; Zhang, B.; Kwong, P.D.; et al. Antibody resistance of SARS-CoV-2 variants B.1.351 and B.1.1.7. Nature 2021, 593, 130–135. [Google Scholar] [CrossRef]
- Pinto, D.; Park, Y.-J.; Beltramello, M.; Walls, A.C.; Tortorici, M.A.; Bianchi, S.; Jaconi, S.; Culap, K.; Zatta, F.; De Marco, A.; et al. Cross-neutralization of SARS-CoV-2 by a human monoclonal SARS-CoV antibody. Nature 2020, 583, 290–295. [Google Scholar] [CrossRef]
- Cathcart, A.L.; Havenar-Daughton, C.; Lempp, F.A.; Ma, D.; Schmid, M.; Agostini, M.L.; Guarino, B.; Di Iulio, J.; Rosen, L.; Tucker, H.; et al. The Dual Function Monoclonal Antibodies VIR-7831 and VIR-7832 Demonstrate Potent in Vitro and in Vivo Activity against SARS-CoV-2. bioRxiv 2021. [Google Scholar] [CrossRef]
- McCallum, M.; Bassi, J.; de Marco, A.; Chen, A.; Walls, A.C.; di Iulio, J.; Tortorici, M.A.; Navarro, M.; Silacci-Fregni, C.; Saliba, C.; et al. SARS-CoV-2 immune evasion by variant B.1.427/B.1.429. bioRxiv 2021. [Google Scholar] [CrossRef]
- Destras, G.; Bal, A.; Simon, B.; Lina, B.; Josset, L. Sotrovimab drives SARS-CoV-2 omicron variant evolution in immunocompromised patients. Lancet Microbe 2022, 3, e559. [Google Scholar] [CrossRef]
- Kim, C.; Ryu, D.-K.; Lee, J.; Kim, Y.-I.; Seo, J.-M.; Kim, Y.-G.; Jeong, J.-H.; Kim, M.; Kim, J.-I.; Kim, P.; et al. A therapeutic neutralizing antibody targeting receptor binding domain of SARS-CoV-2 spike protein. Nat. Commun. 2021, 12, 288. [Google Scholar] [CrossRef]
- Syed, Y.Y. Regdanvimab: First Approval. Drugs 2021, 81, 2133–2137. [Google Scholar] [CrossRef]
- Vanhove, B.; Marot, S.; Gaborit, B.; Evanno, G.; Malet, I.; Ciron, C.; Royer, P.-J.; Lheriteau, E.; Denié, S.; Raffi, F.; et al. XAV-19, a Novel Swine Glyco-Humanized Polyclonal Antibody against SARS-CoV-2 Spike, Efficiently Neutralizes B.1.1.7 British and B.1.351 South-African Variants. bioRxiv 2021. [Google Scholar] [CrossRef]
- Vanhove, B.; Marot, S.; Evanno, G.; Malet, I.; Rouvray, G.; Shneiker, F.; Mevel, E.; Ciron, C.; Rousse, J.; Royer, P.-J.; et al. An-ti-SARS-CoV-2 Swine Glyco-Humanized Polyclonal Antibody XAV-19 Retains Neutralizing Activity against SARS-CoV-2 B.1.1.529 (Omicron). bioRxiv 2022. [Google Scholar] [CrossRef]
- Gaborit, B.; Dailly, E.; Vanhove, B.; Josien, R.; Lacombe, K.; Dubee, V.; Ferre, V.; Brouard, S.; Ader, F.; Vibet, M.A.; et al. Pharmacokinetics and Safety of XAV-19, a Swine Glycohumanized Polyclonal Anti-SARS-CoV-2 Antibody, for COVID-19-Related Moderate Pneumonia: A Randomized, Double-Blind, Placebo-Controlled, Phase IIa Study. Antimicrob Agents Chemother 2021, 65, e01237-21. [Google Scholar] [CrossRef]
- Wang, R.; Zhang, Q.; Ge, J.; Ren, W.; Zhang, R.; Lan, J.; Ju, B.; Su, B.; Yu, F.; Chen, P.; et al. SARS-CoV-2 Variants Resist An-tibody Neutralization and Broaden Host ACE2 Usage. bioRxiv 2021. [Google Scholar] [CrossRef]
- Robbie, G.J.; Criste, R.; Dall’Acqua, W.F.; Jensen, K.; Patel, N.K.; Losonsky, G.A.; Griffin, M.P. A Novel Investigational Fc-Modified Humanized Monoclonal Antibody, Motavizumab-YTE, Has an Extended Half-Life in Healthy Adults. Antimicrob. Agents Chemother. 2013, 57, 6147–6153. [Google Scholar] [CrossRef] [PubMed]
- Saunders, K.O. Conceptual Approaches to Modulating Antibody Effector Functions and Circulation Half-Life. Front. Immunol. 2019, 10, 1296. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, M.C.; Chew, K.W.; Deo, R.; Flynn, J.P.; Regan, J.; Crain, C.R.; Moser, C.; Hughes, M.D.; Ritz, J.; Ribeiro, R.M.; et al. Emergence of SARS-CoV-2 escape mutations during Bamlanivimab therapy in a phase II randomized clinical trial. Nat. Microbiol. 2022, 7, 1906–1917. [Google Scholar] [CrossRef] [PubMed]
- Hao, X.; Zhang, Z.; Ma, J.; Cheng, L.; Ji, Y.; Liu, Y.; Zhao, D.; Zhang, W.; Li, C.; Yan, L.; et al. Randomized, Placebo-Controlled, Single-Blind Phase 1 Studies of the Safety, Tolerability, and Pharmacokinetics of BRII-196 and BRII-198, SARS-CoV-2 Spike-Targeting Monoclonal Antibodies with an Extended Half-Life in Healthy Adults. Front. Pharmacol. 2022, 13, 3679. [Google Scholar] [CrossRef]
- Leader, B.; Baca, Q.J.; Golan, D.E. Protein therapeutics: A summary and pharmacological classification. Nat. Rev. Drug Discov. 2008, 7, 21–39. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, E.C.; Gandhi, T.N.; Petty, L.A. Monoclonal Antibodies for COVID-19. JAMA 2021, 325, 1015. [Google Scholar] [CrossRef]
- Chung, C.H. Managing Premedications and the Risk for Reactions to Infusional Monoclonal Antibody Therapy. Oncology 2008, 13, 725–732. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Nirula, A.; Chen, P.; Boscia, J.; Heller, B.; Morris, J.; Huhn, G.; Cardona, J.; Mocherla, B.; Stosor, V.; et al. Effect of Bamlanivimab as Monotherapy or in Combination With Etesevimab on Viral Load in Patients With Mild to Moderate COVID-19. JAMA 2021, 325, 632–644. [Google Scholar] [CrossRef]
- Chen, P.; Nirula, A.; Heller, B.; Gottlieb, R.L.; Boscia, J.; Morris, J.; Huhn, G.; Cardona, J.; Mocherla, B.; Stosor, V.; et al. SARS-CoV-2 Neutralizing Antibody LY-CoV555 in Outpatients with COVID-19. N. Engl. J. Med. 2021, 384, 229–237. [Google Scholar] [CrossRef]
- Shimizu, J.; Sasaki, T.; Koketsu, R.; Morita, R.; Yoshimura, Y.; Murakami, A.; Saito, Y.; Kusunoki, T.; Samune, Y.; Nakayama, E.E.; et al. Reevaluation of antibody-dependent enhancement of infection in anti-SARS-CoV-2 therapeutic antibodies and mRNA-vaccine antisera using FcR- and ACE2-positive cells. Sci. Rep. 2022, 12, 15612. [Google Scholar] [CrossRef]
- Adhikari, E.H.; SoRelle, J.A.; McIntire, D.D.; Spong, C.Y. Increasing severity of COVID-19 in pregnancy with Delta (B.1.617.2) variant surge. Am. J. Obstet. Gynecol. 2021, 226, 149–151. [Google Scholar] [CrossRef] [PubMed]
- McCreary, E.K.; Lemon, L.; Megli, C.; Oakes, A.; Seymour, C.W.; Beigi, R.; McLaughlin, M.; Simhan, H.; Wiesenfeld, H.; Lau, S.; et al. Monoclonal Antibodies for Treatment of SARS-CoV-2 Infection During Pregnancy A Cohort Study. Ann. Intern. Med. 2022, 175, 1707–1716. [Google Scholar] [CrossRef]
- Hoeltzenbein, M.; Beck, E.; Rajwanshi, R.; Skorpen, C.G.; Berber, E.; Schaefer, C.; Østensen, M. Tocilizumab use in pregnancy: Analysis of a global safety database including data from clinical trials and post-marketing data. Semin. Arthritis Rheum. 2016, 46, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, S.C.; Lapinsky, S.E. Tocilizumab for coronavirus disease 2019 in pregnancy and lactation: A narrative review. Clin. Microbiol. Infect. 2021, 28, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Hubert, P.; Heitzmann, A.; Viel, S.; Nicolas, A.; Sastre-Garau, X.; Oppezzo, P.; Pritsch, O.; Osinaga, E.; Amigorena, S. Antibody-Dependent Cell Cytotoxicity Synapses Form in Mice during Tumor-Specific Antibody Immunotherapy. Cancer Res. 2011, 71, 5134–5143. [Google Scholar] [CrossRef]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef]
- Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Sharma, G.; Lee, S.; Agoramoorthy, G. COVID-19: Consider IL-6 receptor antagonist for the therapy of cytokine storm syndrome in SARS-CoV-2 infected patients. J. Med. Virol. 2020, 92, 2260–2262. [Google Scholar] [CrossRef]
- Gordon, A.C.; Mouncey, P.R.; Al-Beidh, F.; Rowan, K.M.; Nichol, A.D.; Arabi, Y.M.; Annane, D.; Beane, A.; Van Bentum-Puijk, W.; Berry, L.R.; et al. Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [CrossRef]
- Abani, O.; Abbas, A.; Abbas, F.; Abbas, M.; Abbasi, S.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Jones, S.A.; Hunter, C.A. Is IL-6 a key cytokine target for therapy in COVID-19? Nat. Rev. Immunol. 2021, 21, 337–339. [Google Scholar] [CrossRef]
- Reshaping a Human Antibody to Inhibit the Interleukin 6-Dependent Tumor Cell Growth1 |Cancer Research| American Association for Cancer Research. Available online: https://aacrjournals.org/cancerres/article/53/4/851/499662/Reshaping-a-Human-Antibody-to-Inhibit-the (accessed on 30 March 2023).
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. Efficacy of Tocilizumab in Patients Hospitalized with COVID-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Group, R.C.; Horby, P.W.; Pessoa-Amorim, G.; Peto, L.; Brightling, C.E.; Sarkar, R.; Thomas, K.; Jeebun, V.; Ashish, A.; Tully, R.; et al. Tocilizumab in Patients Admitted to Hospital with COVID-19 (RECOVERY): Preliminary Results of a Randomised, Controlled, Open-Label, Platform Trial. medRxiv 2021. [Google Scholar] [CrossRef]
- Tian, J.; Zhang, M.; Jin, M.; Zhang, F.; Chu, Q.; Wang, X.; Chen, C.; Yue, H.; Zhang, L.; Du, R.; et al. Repurposed Tocilizumab in Patients with Severe COVID-19. J. Immunol. 2021, 206, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Pandey, M.; Tuncman, G.; Hotamisligil, G.S.; Samad, F. Divergent Roles for p55 and p75 TNF-α Receptors in the Induction of Plasminogen Activator Inhibitor-1. Am. J. Pathol. 2003, 162, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Markham, A.; Lamb, H.M. Infliximab: A Review of Its Use in the Management of Rheumatoid Arthritis. Drugs 2000, 59, 1341–1359. [Google Scholar] [CrossRef] [PubMed]
- Hachem, H.; Godara, A.; Schroeder, C.; Fein, D.; Mann, H.; Lawlor, C.; Marshall, J.; Klein, A.; Poutsiaka, D.; Breeze, J.L.; et al. Rapid and Sustained Decline in CXCL-10 (IP-10) Annotates Clinical Outcomes Following TNF-α Antagonist Therapy in Hos-pitalized Patients with Severe and Critical COVID-19 Respiratory Failure. medRxiv 2021, 8, S351–S352. [Google Scholar] [CrossRef]
- Sorrell, F.J.; Szklarz, M.; Azeez, K.R.A.; Elkins, J.M.; Knapp, S. Family-wide Structural Analysis of Human Numb-Associated Protein Kinases. Structure 2016, 24, 401–411. [Google Scholar] [CrossRef]
- Martínez Ferrer, A.; Aguilar Zamora, M.; Montolio Chiva, L.; Valls Pascual, E.; Ybáñez García, D.; Alegre Sancho, J.J. Baricitinib En El Tratamiento de La Artritis Reumatoide. Rev. De La SVR Soc. Valencia. De Reumatol. 2017, 7, 17–22. [Google Scholar]
- Bronte, V.; Ugel, S.; Tinazzi, E.; Vella, A.; De Sanctis, F.; Canè, S.; Batani, V.; Trovato, R.; Fiore, A.; Petrova, V.; et al. Baricitinib restrains the immune dysregulation in patients with severe COVID-19. J. Clin. Investig. 2020, 130, 6409–6416. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- Kubo, S.; Nakayamada, S.; Sakata, K.; Kitanaga, Y.; Ma, X.; Lee, S.; Ishii, A.; Yamagata, K.; Nakano, K.; Tanaka, Y. Janus Kinase Inhibitor Baricitinib Modulates Human Innate and Adaptive Immune System. Front. Immunol. 2018, 9, 1510. [Google Scholar] [CrossRef] [PubMed]
- Moura, R.A.; Fonseca, J.E. JAK Inhibitors and Modulation of B Cell Immune Responses in Rheumatoid Arthritis. Front. Med. 2021, 7, 1105. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; McInnes, I.B.; Taylor, P.C.; Byers, N.L.; Chen, L.; de Bono, S.; Issa, M.; Macias, W.L.; Rogai, V.; Rooney, T.P.; et al. Characterization and Changes of Lymphocyte Subsets in Baricitinib-Treated Patients With Rheumatoid Arthritis: An Integrated Analysis. Arthritis Rheumatol. 2018, 70, 1923–1932. [Google Scholar] [CrossRef]
- Guimarães, P.O.; Quirk, D.; Furtado, R.H.; Maia, L.N.; Saraiva, J.F.; Antunes, M.O.; Filho, R.K.; Junior, V.M.; Soeiro, A.M.; Tognon, A.P.; et al. Tofacitinib in Patients Hospitalized with COVID-19 Pneumonia. N. Engl. J. Med. 2021, 385, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Boor, P.P.; de Ruiter, P.; Asmawidjaja, P.S.; Lubberts, E.; van der Laan, L.J.; Kwekkeboom, J. JAK-inhibitor tofacitinib suppresses interferon alfa production by plasmacytoid dendritic cells and inhibits arthrogenic and antiviral effects of interferon alfa. Transl. Res. 2017, 188, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Dowty, M.E.; Lin, T.H.; Jesson, M.I.; Hegen, M.; Martin, D.A.; Katkade, V.; Menon, S.; Telliez, J. Janus kinase inhibitors for the treatment of rheumatoid arthritis demonstrate similar profiles of in vitro cytokine receptor inhibition. Pharmacol. Res. Perspect. 2019, 7, e00537. [Google Scholar] [CrossRef]
- Dhillon, S. Tofacitinib: A Review in Rheumatoid Arthritis. Drugs 2017, 77, 1987–2001. [Google Scholar] [CrossRef]
- Maslennikov, R.; Ivashkin, V.; Vasilieva, E.; Chipurik, M.; Semikova, P.; Semenets, V.; Russkova, T.; Levshina, A.; Grigoriadis, D.; Magomedov, S.; et al. Tofacitinib reduces mortality in coronavirus disease 2019 Tofacitinib in COVID-19. Pulm. Pharmacol. Ther. 2021, 69, 102039. [Google Scholar] [CrossRef]
- Ajayi, S.; Becker, H.; Reinhardt, H.; Engelhardt, M.; Zeiser, R.; von Bubnoff, N.; Wäsch, R. Ruxolitinib. Recent Results Cancer Res. 2018, 212, 119–132. [Google Scholar] [CrossRef]
- Kiladjian, J.-J.; Zachee, P.; Hino, M.; Pane, F.; Masszi, T.; Harrison, C.N.; Mesa, R.; Miller, C.B.; Passamonti, F.; Durrant, S.; et al. Long-term efficacy and safety of ruxolitinib versus best available therapy in polycythaemia vera (RESPONSE): 5-year follow up of a phase 3 study. Lancet Haematol. 2020, 7, e226–e237. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Wei, J.; Zou, L.; Jiang, T.; Wang, G.; Chen, L.; Huang, L.; Meng, F.; Huang, L.; Wang, N.; et al. Ruxolitinib in treatment of severe coronavirus disease 2019 (COVID-19): A multicenter, single-blind, randomized controlled trial. J. Allergy Clin. Immunol. 2020, 146, 137–146.e3. [Google Scholar] [CrossRef]
- Iastrebner, M.; Castro, J.; Garcia Espina, E.; Lettieri, C.; Payaslian, S.; Cuesta, M.C.; Gutierrez Fernandez, P.; Mandrile, A.; Contreras, A.P.; Gervasoni, S.; et al. Ruxolitinib in severe COVID-19: Results of a multicenter, prospective, single arm, open-label clinical study to investigate the efficacy and safety of ruxolitinib in patients with COVID-19 and severe acute respiratory syndrome. Rev. Fac. Cien. Med. 2021, 78, 294. [Google Scholar] [CrossRef]
- Neubauer, A.; Johow, J.; Mack, E.; Burchert, A.; Meyn, D.; Kadlubiec, A.; Torje, I.; Wulf, H.; Vogelmeier, C.F.; Hoyer, J.; et al. The janus-kinase inhibitor ruxolitinib in SARS-CoV-2 induced acute respiratory distress syndrome (ARDS). Leukemia 2021, 35, 2917–2923. [Google Scholar] [CrossRef]
- Maron, D.J.; Fazio, S.; Linton, M.F. Current Perspectives on Statins. Circulation 2000, 101, 207–213. [Google Scholar] [CrossRef]
- Chansrichavala, P.; Chantharaksri, U.; Sritara, P.; Chaiyaroj, S.C. Atorvastatin Attenuates TLR4-Mediated NF-ΚB Activation in a MyD88-Dependent Pathway. Asian Pac. J. Allergy Immunol. 2009, 27, 49–57. [Google Scholar]
- Lee, K.C.H.; Sewa, D.W.; Phua, G.C. Potential role of statins in COVID-19. Int. J. Infect. Dis. 2020, 96, 615–617. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute ARDS Clinical Trials Network; Truwit, J.D.; Bernard, G.R.; Steingrub, J.; Matthay, A.M.; Liu, K.D.; Albertson, E.T.; Brower, R.G.; Shanholtz, C.; Rock, P.; et al. Rosuvastatin for Sepsis-Associated Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2014, 370, 2191–2200. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, D.; Durand, A.; Gleeson, J.; Taccone, F.S. Failure of statins in ARDS: The quest for the “Holy Grail” continues. Minerva Anestesiol. 2016, 82, 1230–1234. [Google Scholar]
- Masana, L.; Correig, E.; Rodríguez-Borjabad, C.; Anoro, E.; Arroyo, J.A.; Jericó, C.; Pedragosa, A.; Miret, M.; Näf, S.; Pardo, A.; et al. Effect of statin therapy on SARS-CoV-2 infection-related mortality in hospitalized patients. Eur. Hear. J.-Cardiovasc. Pharmacother. 2020, 8, 157–164. [Google Scholar] [CrossRef]
- Cvetkovic, R.S.; Keating, G. Anakinra. Biodrugs 2002, 16, 303–311. [Google Scholar] [CrossRef]
- Kyriakoulis, K.G.; Kollias, A.; Poulakou, G.; Kyriakoulis, I.G.; Trontzas, I.P.; Charpidou, A.; Syrigos, K. The Effect of Anakinra in Hospitalized Patients with COVID-19: An Updated Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 4462. [Google Scholar] [CrossRef]
- Petty, F.; Maul, A. Fluvoxamine. In xPharm: The Comprehensive Pharmacology Reference; Elsevier Inc.: Amsterdam, The Netherlands, 2007; pp. 1–5. [Google Scholar] [CrossRef]
- Hashimoto, K. Repurposing of CNS drugs to treat COVID-19 infection: Targeting the sigma-1 receptor. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 249–258. [Google Scholar] [CrossRef]
- Hallifax, D.; Houston, J.B. Saturable Uptake of Lipophilic Amine Drugs into Isolated Hepatocytes: Mechanisms and Consequences for Quantitative Clearance Prediction. Drug Metab. Dispos. 2007, 35, 1325–1332. [Google Scholar] [CrossRef]
- Lenze, E.J.; Mattar, C.; Zorumski, C.F.; Stevens, A.; Schweiger, J.; Nicol, G.E.; Miller, J.P.; Yang, L.; Yingling, M.; Avidan, M.S.; et al. Fluvoxamine vs. Placebo and Clinical Deterioration in Outpatients With Symptomatic COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 2292–2300. [Google Scholar] [CrossRef]
- Reis, G.; Moreira-Silva, E.A.D.S.; Silva, D.C.M.; Thabane, L.; Milagres, A.C.; Ferreira, T.S.; dos Santos, C.V.Q.; Campos, V.H.d.S.; Nogueira, A.M.R.; de Almeida, A.P.F.G.; et al. Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: The TOGETHER randomised, platform clinical trial. Lancet Glob. Health 2022, 10, e42–e51. [Google Scholar] [CrossRef] [PubMed]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients With Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef]
- Pedersen, S.F.; Ho, Y.-C. SARS-CoV-2: A storm is raging. J. Clin. Investig. 2020, 130, 2202–2205. [Google Scholar] [CrossRef] [PubMed]
- Stratton, C.W.; Tang, Y.; Lu, H. Pathogenesis-directed therapy of 2019 novel coronavirus disease. J. Med. Virol. 2020, 93, 1320–1342. [Google Scholar] [CrossRef]
- Kim, J.S.; Jeong, J.S.; Kwon, S.H.; Kim, S.R.; Lee, Y.C. Roles of PI3K pan-inhibitors and PI3K-δ inhibitors in allergic lung inflammation: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 7608. [Google Scholar] [CrossRef] [PubMed]
- Abu Eid, R.; Ahmad, S.; Lin, Y.; Webb, M.; Berrong, Z.; Shrimali, R.; Kumai, T.; Ananth, S.; Rodriguez, P.C.; Celis, E.; et al. Enhanced Therapeutic Efficacy and Memory of Tumor-Specific CD8 T Cells by Ex Vivo PI3K-δ Inhibition. Cancer Res. 2017, 77, 4135–4145. [Google Scholar] [CrossRef]
- Patton, D.T.; Garden, O.A.; Pearce, W.P.; Clough, L.E.; Monk, C.R.; Leung, E.; Rowan, W.C.; Sancho, S.; Walker, L.S.K.; Vanhaesebroeck, B.; et al. Cutting Edge: The Phosphoinositide 3-Kinase p110δ Is Critical for the Function of CD4+CD25+Foxp3+ Regulatory T Cells. J. Immunol. 2006, 177, 6598–6602. [Google Scholar] [CrossRef]
- Ahmad, S.; Abu-Eid, R.; Shrimali, R.; Webb, M.; Verma, V.; Doroodchi, A.; Berrong, Z.; Samara, R.; Rodriguez, P.C.; Mkrtichyan, M.; et al. Differential PI3Kδ Signaling in CD4+ T-cell Subsets Enables Selective Targeting of T Regulatory Cells to Enhance Cancer Immunotherapy. Cancer Res. 2017, 77, 1892–1904. [Google Scholar] [CrossRef]
- Lee, K.S.; Lee, H.K.; Hayflick, J.S.; Lee, Y.C.; Puri, K.D. Inhibition of phosphoinositide 3-kinase δ attenuates allergic airway inflammation and hyperresponsiveness in murine asthma model. FASEB J. 2006, 20, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Puri, K.D.; Doggett, T.A.; Douangpanya, J.; Hou, Y.; Tino, W.T.; Wilson, T.; Graf, T.; Clayton, E.; Turner, M.; Hayflick, J.S.; et al. Mechanisms and implications of phosphoinositide 3-kinase δ in promoting neutrophil trafficking into inflamed tissue. Blood 2004, 103, 3448–3456. [Google Scholar] [CrossRef]
- Palma, G.; Pasqua, T.; Silvestri, G.; Rocca, C.; Gualtieri, P.; Barbieri, A.; De Bartolo, A.; De Lorenzo, A.; Angelone, T.; Avolio, E.; et al. PI3Kδ Inhibition as a Potential Therapeutic Target in COVID-19. Front. Immunol. 2020, 11, 2094. [Google Scholar] [CrossRef]
- Angulo, I.; Vadas, O.; Garçon, F.; Banham-Hall, E.; Plagnol, V.; Leahy, T.R.; Baxendale, H.; Coulter, T.; Curtis, J.; Wu, C.; et al. Phosphoinositide 3-Kinase δ Gene Mutation Predisposes to Respiratory Infection and Airway Damage. Science 2013, 342, 866–871. [Google Scholar] [CrossRef]
- Uko, N.E.; Güner, O.F.; Matesic, D.F.; Bowen, J.P. Akt Pathway Inhibitors. Curr. Top. Med. Chem. 2020, 20, 883–900. [Google Scholar] [CrossRef] [PubMed]
- Daxian, W.; Deming, T. Viral Hepatitis: Hepatitis B & D—A. Experimental. J. Hepatol. 2015, 62 (Suppl. S2), S521. [Google Scholar] [CrossRef]
- Zheng, F.; Zhou, Y.; Zhou, Z.; Ye, F.; Huang, B.; Huang, Y.; Ma, J.; Zuo, Q.; Tan, X.; Xie, J.; et al. SARS-CoV-2 clearance in COVID-19 patients with Novaferon treatment: A randomized, open-label, parallel-group trial. Int. J. Infect. Dis. 2020, 99, 84–91. [Google Scholar] [CrossRef]
- Sassi, F.; Tamone, C.; D’Amelio, P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients 2018, 10, 1656. [Google Scholar] [CrossRef]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef]
- Matsuoka, L.Y.; Ide, L.; Wortsman, J.; Maclaughlin, J.A.; Holick, M.F. Sunscreens Suppress Cutaneous Vitamin D3 Synthesis. J. Clin. Endocrinol. Metab. 1987, 64, 1165–1168. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, L.Y.; Wortsman, J.; Dannenberg, M.J.; Hollis, B.W.; Lu, Z.; Holick, M.F. Clothing prevents ultraviolet-B radiation-dependent photosynthesis of vitamin D3. J. Clin. Endocrinol. Metab. 1992, 75, 1099–1103. [Google Scholar] [CrossRef]
- Jeon, S.-M.; Shin, E.-A. Exploring vitamin D metabolism and function in cancer. Exp. Mol. Med. 2018, 50, 1–14. [Google Scholar] [CrossRef]
- Zittermann, A. Vitamin D and disease prevention with special reference to cardiovascular disease. Prog. Biophys. Mol. Biol. 2006, 92, 39–48. [Google Scholar] [CrossRef]
- Hewison, M. Vitamin D and the intracrinology of innate immunity. Mol. Cell Endocrinol. 2010, 321, 103–111. [Google Scholar] [CrossRef]
- Provvedini, D.M.; Tsoukas, C.D.; Deftos, L.J.; Manolagas, S.C. 1,25-Dihydroxyvitamin D3 Receptors in Human Leukocytes. Science 1983, 221, 1181–1183. [Google Scholar] [CrossRef]
- Maestro, M.A.; Molnár, F.; Mouriño, A.; Carlberg, C. Vitamin D receptor 2016: Novel ligands and structural insights. Expert Opin. Ther. Pat. 2016, 26, 1291–1306. [Google Scholar] [CrossRef] [PubMed]
- Battault, S.; Whiting, S.J.; Peltier, S.L.; Sadrin, S.; Gerber, G.; Maixent, J.M. Vitamin D metabolism, functions and needs: From science to health claims. Eur. J. Nutr. 2012, 52, 429–441. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.S.; Rafison, B.; Witzel, S.; Reyes, R.E.; Shieh, A.; Chun, R.; Zavala, K.; Hewison, M.; Liu, P.T. Regulation of the extrarenal CYP27B1-hydroxylase. J. Steroid Biochem. Mol. Biol. 2014, 144, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Bruce, D.; Froicu, M.; Weaver, V.; Cantorna, M.T. Failure of T cell homing, reduced CD4/CD8αα intraepithelial lymphocytes, and inflammation in the gut of vitamin D receptor KO mice. Proc. Natl. Acad. Sci. USA 2008, 105, 20834–20839. [Google Scholar] [CrossRef] [PubMed]
- Sigmundsdottir, H.; Pan, J.; Debes, G.F.; Alt, C.; Habtezion, A.; Soler, D.; Butcher, E.C. DCs metabolize sunlight-induced vitamin D3 to ‘program’ T cell attraction to the epidermal chemokine CCL27. Nat. Immunol. 2007, 8, 285–293. [Google Scholar] [CrossRef]
- Turrubiates-Hernández, F.J.; Sánchez-Zuno, G.A.; González-Estevez, G.; Hernández-Bello, J.; Macedo-Ojeda, G.; Muñoz-Valle, J.F. Potential immunomodulatory effects of vitamin D in the prevention of severe coronavirus disease 2019: An ally for Latin America (Review). Int. J. Mol. Med. 2021, 47, 32. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.S.; Czajkowsky, D.M.; Islam, A.; Rahman, A. The role of vitamin D in reducing SARS-CoV-2 infection: An update. Int. Immunopharmacol. 2021, 97, 107686. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, P.B. COVID-19 fatalities, latitude, sunlight, and vitamin D. Am. J. Infect. Control 2020, 48, 1042–1044. [Google Scholar] [CrossRef]
- Rhodes, J.M.; Subramanian, S.; Laird, E.; Kenny, R.A. Editorial: Low population mortality from COVID-19 in countries south of latitude 35 degrees North supports vitamin D as a factor determining severity. Aliment. Pharmacol. Ther. 2020, 51, 1434–1437. [Google Scholar] [CrossRef] [PubMed]
- Engelsen, O. The Relationship between Ultraviolet Radiation Exposure and Vitamin D Status. Nutrients 2010, 2, 482–495. [Google Scholar] [CrossRef]
- Hernández, J.L.; Nan, D.; Fernandez-Ayala, M.; García-Unzueta, M.; Hernández-Hernández, M.A.; López-Hoyos, M.; Muñoz-Cacho, P.; Olmos, J.M.; Gutiérrez-Cuadra, M.; Ruiz-Cubillán, J.J.; et al. Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection. J. Clin. Endocrinol. Metab. 2021, 106, e1343–e1353. [Google Scholar] [CrossRef] [PubMed]
- D’avolio, A.; Avataneo, V.; Manca, A.; Cusato, J.; De Nicolò, A.; Lucchini, R.; Keller, F.; Cantù, M. 25-Hydroxyvitamin D Concentrations Are Lower in Patients with Positive PCR for SARS-CoV-2. Nutrients 2020, 12, 1359. [Google Scholar] [CrossRef]
- Kaufman, H.W.; Niles, J.K.; Kroll, M.H.; Bi, C.; Holick, M.F. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS ONE 2020, 15, e0239252. [Google Scholar] [CrossRef]
- Marcinowska-Suchowierska, E.; Kupisz-Urbańska, M.; Łukaszkiewicz, J.; Płudowski, P.; Jones, G. Vitamin D Toxicity–A Clinical Perspective. Front. Endocrinol. 2018, 9, 550. [Google Scholar] [CrossRef]
- Entrenas Castillo, M.E.; Entrenas Costa, L.M.E.; Vaquero Barrios, J.M.V.; Alcalá Díaz, J.F.A.; López Miranda, J.L.; Bouillon, R.; Quesada Gomez, J.M.Q. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Varna, V.P.; Sharma, U.; Mavalankar, D. Does Vitamin D Supplementation Reduce COVID-19 Severity?: A Systematic Review. QJM Int. J. Med. 2022, 115, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Bignardi, P.R.; Castello, P.D.A.; Aquino, B.D.M.; Delfino, V.D. AIs the Vitamin D Status of Patients with COVID-19 Associated with Reduced Mortality? A Systematic Review and Meta-Analysis. Arch. Endocrinol. Metab. 2023, 67, 276–288. [Google Scholar] [CrossRef] [PubMed]
- Vimaleswaran, K.S.; Forouhi, N.G.; Khunti, K. Vitamin D and COVID-19. BMJ 2021, 372, n544. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Genovese, M.C.; Takeuchi, T.; Hyslop, D.L.; Macias, W.L.; Rooney, T.; Chen, L.; Dickson, C.L.; Camp, J.R.; Cardillo, T.E.; et al. Safety Profile of Baricitinib in Patients with Active Rheumatoid Arthritis with over 2 Years Median Time in Treatment. J. Rheumatol. 2018, 46, 7–18. [Google Scholar] [CrossRef]
- Taylor, P.C.; Weinblatt, M.E.; Burmester, G.R.; Rooney, T.P.; Witt, S.; Walls, C.D.; Issa, M.; Salinas, C.A.; Saifan, C.; Zhang, X.; et al. Cardiovascular Safety During Treatment With Baricitinib in Rheumatoid Arthritis. Arthritis Rheumatol. 2019, 71, 1042–1055. [Google Scholar] [CrossRef]
- Costanzo, G.; Firinu, D.; Losa, F.; Deidda, M.; Barca, M.P.; Del Giacco, S. Baricitinib exposure during pregnancy in rheumatoid arthritis. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1–3. [Google Scholar] [CrossRef]
- Adhyaru, B.B.; Jacobson, T.A. Safety and efficacy of statin therapy. Nat. Rev. Cardiol. 2018, 15, 757–769. [Google Scholar] [CrossRef] [PubMed]
- Benfield, P.; Ward, A. Fluvoxamine: A Review of Its Pharmacodynamic and Pharmacokinetic Properties, and Therapeutic Efficacy in Depressive Illness. Drugs 1986, 32, 313–334. [Google Scholar] [CrossRef] [PubMed]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential effects of coronaviruses on the cardiovascular system: A review. JAMA Cardiol. 2020, 5, 831–840. [Google Scholar] [CrossRef]
- Driggin, E.; Madhavan, M.V.; Gupta, A. The role of vitamin D in cardiovascular disease and COVID-19. Rev. Endocr. Metab. Disord. 2022, 23, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Qiao, G.; Uskokovic, M.; Xiang, W.; Zheng, W.; Kong, J. Vitamin D: A negative endocrine regulator of the renin–angiotensin system and blood pressure. J. Steroid Biochem. Mol. Biol. 2004, 89–90, 387–392. [Google Scholar] [CrossRef] [PubMed]
- V’Kovski, P.; Kratzel, A.; Steiner, S.; Stalder, H.; Thiel, V. Coronavirus biology and replication: Implications for SARS-CoV-2. Nat. Rev. Microbiol. 2021, 19, 155–170. [Google Scholar] [CrossRef]
- Wang, M.-Y.; Zhao, R.; Gao, L.-J.; Gao, X.-F.; Wang, D.-P.; Cao, J.-M. SARS-CoV-2: Structure, Biology, and Structure-Based Therapeutics Development. Front. Cell Infect. Microbiol. 2020, 10, 587269. [Google Scholar] [CrossRef]
- Harrison, A.G.; Lin, T.; Wang, P. Mechanisms of SARS-CoV-2 Transmission and Pathogenesis. Trends Immunol. 2020, 41, 1100–1115. [Google Scholar] [CrossRef]
- Ansems, K.; Grundeis, F.; Dahms, K.; Mikolajewska, A.; Thieme, V.; Piechotta, V.; Metzendorf, M.-I.; Stegemann, M.; Benstoem, C.; Fichtner, F. Remdesivir for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 8, CD014962. [Google Scholar] [CrossRef]
- Hung, I.F.-N.; Lung, K.-C.; Tso, E.Y.-K.; Liu, R.; Chung, T.W.-H.; Chu, M.-Y.; Ng, Y.-Y.; Lo, J.; Chan, J.; Tam, A.R.; et al. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, phase 2 trial. Lancet 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- Solaymani-Dodaran, M.; Ghanei, M.; Bagheri, M.; Qazvini, A.; Vahedi, E.; Saadat, S.H.; Setarehdan, S.A.; Ansarifar, A.; Biganeh, H.; Mohazzab, A.; et al. Safety and efficacy of Favipiravir in moderate to severe SARS-CoV-2 pneumonia. Int. Immunopharmacol. 2021, 95, 107522. [Google Scholar] [CrossRef]
- Arribas, J.R.; Bhagani, S.; Lobo, S.M.; Khaertynova, I.; Mateu, L.; Fishchuk, R.; Park, W.Y.; Hussein, K.; Kim, S.W.; Ghosn, J.; et al. Randomized Trial of Molnupiravir or Placebo in Patients Hospitalized with COVID-19. NEJM Évid. 2022, 1, 2. [Google Scholar] [CrossRef]
- Efficacy and Safety of Direct Anti HCV Drugs in the Treatment of SARS-CoV-2 (COVID-19)—No Study Results Post-ed—ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/ct2/show/results/NCT04535869?cond=NCT04535869&draw=2&rank=1 (accessed on 30 March 2023).
- Jorgensen, S.C.J.; Kebriaei, R.; Dresser, L.D. Remdesivir: Review of Pharmacology, Pre-Clinical Data, and Emerging Clinical Experience for COVID-19. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 659–671. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.X.J.; Cho, S.; Meyyur Aravamudan, V.; Sanda, H.Y.; Palraj, R.; Molton, J.S.; Venkatachalam, I. Remdesivir in Coronavirus Disease 2019 (COVID-19) Treatment: A Review of Evidence. Infection 2021, 49, 401. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Singh, A.; Singh, R.; Misra, A. Remdesivir in COVID-19: A Critical Review of Pharmacology, Pre-Clinical and Clinical Studies. Diabetes Metab. Syndr. 2020, 14, 641. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in Adults with Severe COVID-19: A Randomised, Double-Blind, Placebo-Controlled, Multicentre Trial. Lancet 2020, 395, 1569. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.D.; Lye, D.C.B.; Hui, D.S.; Marks, K.M.; Bruno, R.; Montejano, R.; Spinner, C.D.; Galli, M.; Ahn, M.-Y.; Nahass, R.G.; et al. Remdesivir for 5 or 10 Days in Patients with Severe COVID-19. N. Engl. J. Med. 2020, 383, 1827–1837. [Google Scholar] [CrossRef] [PubMed]
- A Olender, S.; Perez, K.K.; Go, A.S.; Balani, B.; Price-Haywood, E.G.; Shah, N.S.; Wang, S.; Walunas, T.L.; Swaminathan, S.; Slim, J.; et al. Remdesivir for Severe Coronavirus Disease 2019 (COVID-19) Versus a Cohort Receiving Standard of Care. Clin. Infect. Dis. 2020, 73, e4166–e4174. [Google Scholar] [CrossRef] [PubMed]
- Ader, F.; Bouscambert-Duchamp, M.; Hites, M.; Peiffer-Smadja, N.; Poissy, J.; Belhadi, D.; Diallo, A.; Lê, M.-P.; Peytavin, G.; Staub, T.; et al. Remdesivir plus standard of care versus standard of care alone for the treatment of patients admitted to hospital with COVID-19 (DisCoVeRy): A phase 3, randomised, controlled, open-label trial. Lancet Infect. Dis. 2021, 22, 209–221. [Google Scholar] [CrossRef]
- Ali, K.; Azher, T.; Baqi, M.; Binnie, A.; Borgia, S.; Carrier, F.M.; Cavayas, Y.A.; Chagnon, N.; Cheng, M.P.; Conly, J.; et al. Remdesivir for the treatment of patients in hospital with COVID-19 in Canada: A randomized controlled trial. Can. Med. Assoc. J. 2022, 194, E242–E251. [Google Scholar] [CrossRef]
- Khalili, J.S.; Zhu, H.; Mak, N.S.A.; Yan, Y.; Zhu, Y. Novel coronavirus treatment with ribavirin: Groundwork for an evaluation concerning COVID-19. J. Med. Virol. 2020, 92, 740–746. [Google Scholar] [CrossRef]
- Ramírez-Olivencia, G.; Estébanez, M.; Membrillo, F.J.; Ybarra, M.D.C. Uso de ribavirina en virus distintos de la hepatitis C. Una revisión de la evidencia. Enferm. Infecc. Microbiol. Clin. 2018, 37, 602–608. [Google Scholar] [CrossRef]
- Loustaud-Ratti, V.; Debette-Gratien, M.; Jacques, J.; Alain, S.; Marquet, P.; Sautereau, D.; Rousseau, A.; Carrier, P. Ribavirin: Past, present and future. World J. Hepatol. 2016, 8, 123–130. [Google Scholar] [CrossRef]
- Elalfy, H.; Besheer, T.; El-Mesery, A.; El-Gilany, A.; Soliman, M.A.; Alhawarey, A.; Alegezy, M.; Elhadidy, T.; Hewidy, A.A.; Zaghloul, H.; et al. Effect of a combination of nitazoxanide, ribavirin, and ivermectin plus zinc supplement (MANS.NRIZ study) on the clearance of mild COVID-19. J. Med. Virol. 2021, 93, 3176–3183. [Google Scholar] [CrossRef] [PubMed]
- Udwadia, Z.F.; Singh, P.; Barkate, H.; Patil, S.; Rangwala, S.; Pendse, A.; Kadam, J.; Wu, W.; Caracta, C.F.; Tandon, M. Efficacy and safety of favipiravir, an oral RNA-dependent RNA polymerase inhibitor, in mild-to-moderate COVID-19: A randomized, comparative, open-label, multicenter, phase 3 clinical trial. Int. J. Infect. Dis. 2020, 103, 62–71. [Google Scholar] [CrossRef]
- Zhao, H.; Zhang, C.; Zhu, Q.; Chen, X.; Chen, G.; Sun, W.; Xiao, Z.; Du, W.; Yao, J.; Li, G.; et al. Favipiravir in the treatment of patients with SARS-CoV-2 RNA recurrent positive after discharge: A multicenter, open-label, randomized trial. Int. Immunopharmacol. 2021, 97, 107702. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Arora, M.K.; Asdaq, S.M.B.; Alam Khan, S.; Alaqel, S.I.; Alshammari, M.K.; Alshehri, M.M.; Alshrari, A.S.; Ali, A.M.; Al-Shammeri, A.M.; et al. Discovery, Development, and Patent Trends on Molnupiravir: A Prospective Oral Treatment for COVID-19. Molecules 2021, 26, 5795. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, S.M.R.; Pourhanifeh, M.H.; Hamblin, M.R.; Shahrzad, M.K.; Mirzaei, H. RdRp inhibitors and COVID-19: Is molnupiravir a good option? Biomed. Pharmacother. 2021, 146, 112517. [Google Scholar] [CrossRef] [PubMed]
- Pourkarim, F.; Pourtaghi-Anvarian, S.; Rezaee, H. Molnupiravir: A new candidate for COVID-19 treatment. Pharmacol. Res. Perspect. 2022, 10, e00909. [Google Scholar] [CrossRef]
- Fischer, W.A.; Eron, J.J.; Holman, W.; Cohen, M.S.; Fang, L.; Szewczyk, L.J.; Sheahan, T.P.; Baric, R.; Mollan, K.R.; Wolfe, C.R.; et al. A Phase 2a Clinical Trial of Molnupiravir in Patients with COVID-19 Shows Accelerated SARS-CoV-2 RNA Clearance and Elimination of Infectious Virus. Sci. Transl. Med. 2022, 14, 7430. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef]
- Gandhi, Y.; Eley, T.; Fura, A.; Li, W.; Bertz, R.J.; Garimella, T. Daclatasvir: A Review of Preclinical and Clinical Pharmacoki-netics. Clin. Pharmacokinet. 2018, 57, 911–928. [Google Scholar] [CrossRef] [PubMed]
- Nourian, A.; Khalili, H. Sofosbuvir as a Potential Option for the Treatment of COVID-19. Acta Bio. Med. Atenei Parm. 2020, 91, 239. [Google Scholar] [CrossRef]
- Gupta, R.; Dhamija, P. Sofosbuvir for COVID-19 infection: A potential candidate. Indian J. Pharmacol. 2020, 52, 232–233. [Google Scholar] [CrossRef] [PubMed]
- Shabani, M.; Ehdaei, B.S.; Fathi, F.; Dowran, R. A mini-review on sofosbuvir and daclatasvir treatment in coronavirus disease 2019. New Microbes New Infect. 2021, 42, 100895. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, A.; Asgari, A.A.; Norouzi, A.; Kheiri, Z.; Anushirvani, A.; Montazeri, M.; Hosamirudsai, H.; Afhami, S.; Akbarpour, E.; Aliannejad, R.; et al. Sofosbuvir and daclatasvir compared with standard of care in the treatment of patients admitted to hospital with moderate or severe coronavirus infection (COVID-19): A randomized controlled trial. J. Antimicrob. Chemother. 2020, 75, 3379–3385. [Google Scholar] [CrossRef]
- Eslami, G.; Mousaviasl, S.; Radmanesh, E.; Jelvay, S.; Bitaraf, S.; Simmons, B.; Wentzel, H.; Hill, A.; Sadeghi, A.; Freeman, J.; et al. The impact of sofosbuvir/daclatasvir or ribavirin in patients with severe COVID-19. J. Antimicrob. Chemother. 2020, 75, 3366–3372. [Google Scholar] [CrossRef]
- El-Bendary, M.; Abd-Elsalam, S.; Elbaz, T.; El-Akel, W.; Cordie, A.; Elhadidy, T.; Elalfy, H.; Farid, K.; Elegezy, M.; El-Badrawy, A.; et al. RETRACTED ARTICLE: Efficacy of combined Sofosbuvir and Daclatasvir in the treatment of COVID-19 patients with pneumonia: A multicenter Egyptian study. Expert Rev. Anti-Infect. Ther. 2021, 20, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Mobarak, S.; Salasi, M.; Hormati, A.; Khodadadi, J.; Ziaee, M.; Abedi, F.; Ebrahimzadeh, A.; Azarkar, Z.; Mansour-Ghanaei, F.; Joukar, F.; et al. Evaluation of the effect of sofosbuvir and daclatasvir in hospitalized COVID-19 patients: A randomized double-blind clinical trial (DISCOVER). J. Antimicrob. Chemother. 2021, 77, 758–766. [Google Scholar] [CrossRef]
- Jonny, S.C.; Violetta, L.; Kartasasmita, A.S.; Roesli, R.M.A.; Rita, C. Pharmacological Treatment Options for Coronavirus Disease-19 in Renal Patients. Int. J. Nephrol. 2021, 2021, 4078713. [Google Scholar] [CrossRef]
- Jorgensen, S.C.; Tabbara, N.; Burry, L. A review of COVID-19 therapeutics in pregnancy and lactation. Obstet. Med. 2022, 15, 225–232. [Google Scholar] [CrossRef]
- Koshi, E.; Saito, S.; Okazaki, M.; Toyama, Y.; Ishimoto, T.; Kosugi, T.; Hiraiwa, H.; Jingushi, N.; Yamamoto, T.; Ozaki, M.; et al. Efficacy of favipiravir for an end stage renal disease patient on maintenance hemodialysis infected with novel coronavirus disease 2019. CEN Case Rep. 2020, 10, 126–131. [Google Scholar] [CrossRef]
- Hayden, F.G.; Shindo, N. Influenza virus polymerase inhibitors in clinical development. Curr. Opin. Infect. Dis. 2019, 32, 176–186. [Google Scholar] [CrossRef]
- Naseri, A.; Sahebari, S.S.; Hosseini, M.-S. Pharmacotherapy of COVID-19: Considerations for Pregnancy and Breastfeeding. J. Obstet. Gynecol. Cancer Res. 2022, 7, 1–6. [Google Scholar] [CrossRef]
- Hessel, M.H.M.; Cohen, A.F.; Rissmann, R. Sofosbuvir and daclatasvir. Br. J. Clin. Pharmacol. 2016, 82, 878–879. [Google Scholar] [CrossRef]
- Waters, M.D.; Warren, S.; Hughes, C.; Lewis, P.; Zhang, F. Human genetic risk of treatment with antiviral nucleoside analog drugs that induce lethal mutagenesis: The special case of molnupiravir. Environ. Mol. Mutagen. 2022, 63, 37–63. [Google Scholar] [CrossRef]
- Zhou, S.; Hill, C.S.; Sarkar, S.; Tse, L.V.; Woodburn, B.M.D.; Schinazi, R.F.; Sheahan, T.P.; Baric, R.S.; Heise, M.T.; Swanstrom, R. β-d-N4-hydroxycytidine Inhibits SARS-CoV-2 Through Lethal Mutagenesis But Is Also Mutagenic To Mammalian Cells. J. Infect. Dis. 2021, 224, 415–419. [Google Scholar] [CrossRef]
- Goldman, J.D.; Gonzalez, M.A.; Rüthrich, M.M.; Sharon, E.; von Lilienfeld-Toal, M. COVID-19 and Cancer: Special Considerations for Patients Receiving Immunotherapy and Immunosuppressive Cancer Therapies. Am. Soc. Clin. Oncol. Educ. Book 2022, 42, 176–188. [Google Scholar] [CrossRef]
- Villar, J.; Belda, J.; Añón, J.M.; Blanco, J.; Pérez-Méndez, L.; Ferrando, C.; Martínez, D.; Soler, J.A.; Ambrós, A.; Muñoz, T.; et al. Evaluating the efficacy of dexamethasone in the treatment of patients with persistent acute respiratory distress syndrome: Study protocol for a randomized controlled trial. Trials 2016, 17, 342. [Google Scholar] [CrossRef]
- Comparison of Efficacy of Dexamethasone and Methylprednisolone in Moderate to Severe COVID 19 Disease—Full Text View—ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04603729?cond=NCT04603729&draw=2&rank=1 (accessed on 30 March 2023).
- Ahmed, M.H.; Hassan, A. Dexamethasone for the Treatment of Coronavirus Disease (COVID-19): A Review. SN Compr. Clin. Med. 2020, 2, 2637–2646. [Google Scholar] [CrossRef]
- Romanou, V.; Koukaki, E.; Chantziara, V.; Stamou, P.; Kote, A.; Vasileiadis, I.; Koutsoukou, A.; Rovina, N. Dexamethasone in the Treatment of COVID-19: Primus Inter Pares? J. Pers. Med. 2021, 11, 556. [Google Scholar] [CrossRef]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.V.A.O.; et al. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients With Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef] [PubMed]
- The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Durr, K.M.; Hendin, A.; Perry, J.J. Effect of 12 mg vs. 6 mg of dexamethasone on the number of days alive without life support in adults with COVID-19 and severe hypoxemia: The COVID STEROID 2 randomized trial. Can. J. Emerg. Med. 2022, 24, 266–267. [Google Scholar] [CrossRef]
- Toroghi, N.; Abbasian, L.; Nourian, A.; Davoudi-Monfared, E.; Khalili, H.; Hasannezhad, M.; Ghiasvand, F.; Jafari, S.; Emadi-Kouchak, H.; Yekaninejad, M.S. Comparing efficacy and safety of different doses of dexamethasone in the treatment of COVID-19: A three-arm randomized clinical trial. Pharmacol. Rep. 2021, 74, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Maskin, L.P.; Bonelli, I.; Olarte, G.L.; Palizas, J.F.; E Velo, A.; Lurbet, M.F.; Lovazzano, P.; Kotsias, S.; Attie, S.; Saubidet, I.L.; et al. High- Versus Low-Dose Dexamethasone for the Treatment of COVID-19-Related Acute Respiratory Distress Syndrome: A Multicenter, Randomized Open-Label Clinical Trial. J. Intensiv. Care Med. 2021, 37, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Wang, L.; Kuo, H.-C.D.; Shannar, A.; Peter, R.; Chou, P.J.; Li, S.; Hudlikar, R.; Liu, X.; Liu, Z.; et al. An Update on Current Therapeutic Drugs Treating COVID-19. Curr. Pharmacol. Rep. 2020, 6, 56–70. [Google Scholar] [CrossRef]
- Ocejo, A.; Correa, R. Methylprednisolone. In xPharm: The Comprehensive Pharmacology Reference; Elsevier Inc.: Amsterdam, The Netherlands, 2007; pp. 1–6. [Google Scholar] [CrossRef]
- Edalatifard, M.; Akhtari, M.; Salehi, M.; Naderi, Z.; Jamshidi, A.; Mostafaei, S.; Najafizadeh, S.R.; Farhadi, E.; Jalili, N.; Esfahani, M.; et al. Intravenous methylprednisolone pulse as a treatment for hospitalised severe COVID-19 patients: Results from a randomised controlled clinical trial. Eur. Respir. J. 2020, 56, 2002808. [Google Scholar] [CrossRef]
- Corral-Gudino, L.; GLUCOCOVID investigators; Bahamonde, A.; Arnaiz-Revillas, F.; Gómez-Barquero, J.; Abadía-Otero, J.; García-Ibarbia, C.; Mora, V.; Cerezo-Hernández, A.; Hernández, J.L.; et al. Methylprednisolone in Adults Hospitalized with COVID-19 Pneumonia: An Open-Label Randomized Trial (GLUCOCOVID). Wien. Klin. Wochenschr. 2021, 133, 303–311. [Google Scholar] [CrossRef]
- Jeronimo, C.M.P.; Farias, M.E.L.; Val, F.F.A.; Sampaio, V.S.; Alexandre, M.A.A.; Melo, G.C.; Safe, I.P.; Borba, M.G.S.; Netto, R.L.A.; Maciel, A.B.S.; et al. Methylprednisolone as Adjunctive Therapy for Patients Hospitalized with Coronavirus Disease 2019 (COVID-19; MetCOVID): A Randomized, Double-blind, Phase IIb, Placebo-controlled Trial. Clin. Infect. Dis. 2020, 72, e373–e381. [Google Scholar] [CrossRef]
- BATIREL, A.; Demirhan, R.; Eser, N.; Körlü, E.; Tezcan, M.E. Pulse steroid treatment for hospitalized adults with COVID-19. Turk. J. Med. Sci. 2021, 51, 2248–2255. [Google Scholar] [CrossRef]
- Pinzón, M.A.; Ortiz, S.; Holguín, H.; Betancur, J.F.; Cardona Arango, D.; Laniado, H.; Arias, C.A.; Muñoz, B.; Quiceno, J.; Jaramillo, D.; et al. Dexamethasone vs. methylprednisolone high dose for COVID-19 pneumonia. PLoS ONE 2021, 16, e0252057. [Google Scholar] [CrossRef] [PubMed]
- Ranjbar, K.; Moghadami, M.; Mirahmadizadeh, A.; Fallahi, M.J.; Khaloo, V.; Shahriarirad, R.; Erfani, A.; Khodamoradi, Z.; Saadi, M.H.G. Methylprednisolone or dexamethasone, which one is superior corticosteroid in the treatment of hospitalized COVID-19 patients: A triple-blinded randomized controlled trial. BMC Infect. Dis. 2021, 21, 337. [Google Scholar] [CrossRef]
- Patel, C.; Parmar, K.; Patel, D.; Patel, S.; Sheth, D.; Beladiya, J.V. Effect of corticosteroid therapy on mortality in COVID-19 patients—A systematic review and meta-analysis. Rev. Med. Virol. 2022, 32, e2386. [Google Scholar] [CrossRef]
- Prentice, R.E.; Al-Ani, A.; Christensen, B. Managing COVID -19 in patients with inflammatory bowel disease: Navigating unprecedented challenges. Intern. Med. J. 2021, 51, 284–287. [Google Scholar] [CrossRef]
- Chen, F.; Hao, L.; Zhu, S.; Yang, X.; Shi, W.; Zheng, K.; Wang, T.; Chen, H. Potential Adverse Effects of Dexamethasone Therapy on COVID-19 Patients: Review and Recommendations. Infect. Dis. Ther. 2021, 10, 1907–1931. [Google Scholar] [CrossRef]
- Kadam, S.B.; Sukhramani, G.S.; Bishnoi, P.; Pable, A.A.; Barvkar, V.T. SARS-CoV-2, the pandemic coronavirus: Molecular and structural insights. J. Basic Microbiol. 2021, 61, 180–202. [Google Scholar] [CrossRef]
- Saadat, Y.R.; Khatibi, S.M.H.; Vahed, S.Z.; Ardalan, M. Host Serine Proteases: A Potential Targeted Therapy for COVID-19 and Influenza. Front. Mol. Biosci. 2021, 8, 725528. [Google Scholar] [CrossRef]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef]
- Comparison of Lopinavir/Ritonavir or Hydroxychloroquine in Patients With Mild Coronavirus Disease (COVID-19)—No Study Results Posted—ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/ct2/show/results/NCT04307693?cond=NCT04307693&draw=2&rank=1 (accessed on 30 March 2023).
- Chupp, G.; Spichler-Moffarah, A.; Søgaard, O.S.; Esserman, D.; Dziura, J.; Danzig, L.; Chaurasia, R.; Patra, K.P.; Salovey, A.; Nunez, A.; et al. A Phase 2 Randomized, Double-Blind, Placebo-Controlled Trial of Oral Camostat Mesylate for Early Treatment of COVID-19 Outpatients Showed Shorter Illness Course and Attenuation of Loss of Smell and Taste. medRxiv 2022. [Google Scholar] [CrossRef]
- Alpha-1-Antitrypsin-Deficiency in COVID-19—Full Text View—ClinicalTrials.Gov. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04799873 (accessed on 30 March 2023).
- Lamb, Y.N. Nirmatrelvir Plus Ritonavir: First Approval. Drugs 2022, 82, 585–591. [Google Scholar] [CrossRef]
- McDonald, E.G.; Lee, T.C. Association nirmatrelvir/ritonavir contre la COVID-19. Can. Med. Assoc. J. 2022, 194, E365–E366. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, L. In the age of Omicron variant: Paxlovid raises new hopes of COVID-19 recovery. J. Med. Virol. 2021, 94, 1766–1767. [Google Scholar] [CrossRef]
- Singh, R.S.P.; Toussi, S.S.; Hackman, F.; Chan, P.L.; Rao, R.; Allen, R.; Van Eyck, L.; Pawlak, S.; Kadar, E.P.; Clark, F.; et al. Innovative Randomized Phase I Study and Dosing Regimen Selection to Accelerate and Inform Pivotal COVID-19 Trial of Nirmatrelvir. Clin. Pharmacol. Ther. 2022, 112, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of Paxlovid in Reducing Severe Coronavirus Disease 2019 and Mortality in High-Risk Patients. Clin. Infect. Dis. 2022, 76, e342–e349. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.; Chen, C.; Tang, J.; Wang, C.; Zhou, M.; Cheng, Y.; Zhou, X.; Wu, Q.; Zhang, X.; Feng, Z.; et al. Efficacy and safety of three new oral antiviral treatment (molnupiravir, fluvoxamine and Paxlovid) for COVID-19: A meta-analysis. Ann. Med. 2022, 54, 516–523. [Google Scholar] [CrossRef]
- Extance, A. COVID-19: What is the evidence for the antiviral Paxlovid? BMJ 2022, 377, o1037. [Google Scholar] [CrossRef]
- Ullrich, S.; Ekanayake, K.B.; Otting, G.; Nitsche, C. Main Protease Mutants of SARS-CoV-2 Variants Remain Susceptible to Nirmatrelvir (PF-07321332). bioRxiv 2022. [Google Scholar] [CrossRef]
- Trivedi, N.; Verma, A.; Kumar, D. Possible treatment and strategies for COVID-19: Review and assessment. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 12593–12608. [Google Scholar]
- Uzunova, K.; Filipova, E.; Pavlova, V.; Vekov, T. Insights into antiviral mechanisms of remdesivir, lopinavir/ritonavir and chloroquine/hydroxychloroquine affecting the new SARS-CoV-2. Biomed. Pharmacother. 2020, 131, 110668. [Google Scholar] [CrossRef]
- Magro, P.; Zanella, I.; Pescarolo, M.; Castelli, F.; Quiros-Roldan, E. Lopinavir/ritonavir: Repurposing an old drug for HIV infection in COVID-19 treatment. Biomed. J. 2020, 44, 43–53. [Google Scholar] [CrossRef]
- Horby, P.W.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Emberson, J.; Palfreeman, A.; Raw, J.; Elmahi, E.; Prudon, B.; et al. Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe COVID-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Ader, F.; Peiffer-Smadja, N.; Poissy, J.; Bouscambert-Duchamp, M.; Belhadi, D.; Diallo, A.; Delmas, C.; Saillard, J.; Dechanet, A.; Mercier, N.; et al. An open-label randomized controlled trial of the effect of lopinavir/ritonavir, lopinavir/ritonavir plus IFN-β-1a and hydroxychloroquine in hospitalized patients with COVID-19. Clin. Microbiol. Infect. 2021, 27, 1826–1837. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Gordon, A.C.; Derde, L.P.G.; Nichol, A.D.; Murthy, S.; Al Beidh, F.; Annane, D.; Al Swaidan, L.; Beane, A.; Beasley, R.; et al. Lopinavir-ritonavir and hydroxychloroquine for critically ill patients with COVID-19: REMAP-CAP randomized controlled trial. Intensiv. Care Med. 2021, 47, 867–886. [Google Scholar] [CrossRef]
- Vimberg, V. Teicoplanin—A New Use for an Old Drug in the COVID-19 Era? Pharmaceuticals 2021, 14, 1227. [Google Scholar] [CrossRef]
- Yasar, Z.; Yemisen, M.; Yasar, H.; Ertaş, A.; Meric, K.; Sahin, S. Can treatment with teicoplanin improve the prognosis of COVID-19 patients? Int. J. Clin. Pract. 2021, 75, e14752. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Alessandri, F.; D’Ettorre, G.; Borrazzo, C.; Spagnolello, O.; Oliva, A.; Ruberto, F.; Mastroianni, C.M.; Pugliese, F.; Venditti, M. Is teicoplanin a complementary treatment option for COVID-19? The question remains. Int. J. Antimicrob. Agents 2020, 56, 106029. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, G.; Alessandri, F.; Oliva, A.; Borrazzo, C.; Dell’Isola, S.; Ialungo, A.M.; Rastrelli, E.; Pelli, M.; Raponi, G.; Turriziani, O.; et al. The role of teicoplanin in the treatment of SARS-CoV-2 infection: A retrospective study in critically ill COVID-19 patients (Tei-COVID study). J. Med. Virol. 2021, 93, 4319–4325. [Google Scholar] [CrossRef]
- Breining, P.; Frølund, A.L.; Højen, J.F.; Gunst, J.D.; Staerke, N.B.; Saedder, E.; Cases-Thomas, M.; Little, P.; Nielsen, L.P.; Søgaard, O.S.; et al. Camostat mesylate against SARS-CoV-2 and COVID-19—Rationale, dosing and safety. Basic Clin. Pharmacol. Toxicol. 2020, 128, 204–212. [Google Scholar] [CrossRef]
- Gunst, J.D.; Staerke, N.B.; Pahus, M.H.; Kristensen, L.H.; Bodilsen, J.; Lohse, N.; Dalgaard, L.S.; Brønnum, D.; Fröbert, O.; Hønge, B.; et al. Efficacy of the TMPRSS2 inhibitor camostat mesilate in patients hospitalized with COVID-19-a double-blind randomized controlled trial. Eclinicalmedicine 2021, 35, 100849. [Google Scholar] [CrossRef]
- Uno, Y. Camostat mesilate therapy for COVID-19. Intern. Emerg. Med. 2020, 15, 1577–1578. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Bensasi, H.; Taha, A.; Bauer, M.; Ismail, K.; Belhaj, G.; Afet, K.M.; Munde, D.; Monk, D.; Buschbeck, S.; et al. Camostat mesylate therapy in critically ill patients with COVID-19 pneumonia. Intensiv. Care Med. 2021, 47, 707–709. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Keshavjee, S.; Liu, M. Alpha-1 Antitrypsin for COVID-19 Treatment: Dual Role in Antiviral Infection and Anti-Inflammation. Front. Pharmacol. 2020, 11, 615398. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Hippensteel, J.; Leavitt, A.; Maloney, J.P.; Beckham, D.; Garcia, C.; Li, Q.; Freed, B.M.; Ordway, D.; Sandhaus, R.A.; et al. Hypothesis: Alpha-1-antitrypsin is a promising treatment option for COVID-19. Med. Hypotheses 2020, 146, 110394. [Google Scholar] [CrossRef] [PubMed]
- de Loyola, M.B.; dos Reis, T.T.A.; de Oliveira, G.X.L.M.; Palmeira, J.D.F.; Argañaraz, G.A.; Argañaraz, E.R. Alpha-1-antitrypsin: A possible host protective factor against COVID-19. Rev. Med. Virol. 2020, 31, e2157. [Google Scholar] [CrossRef]
- Strassmair, M.; Stangl, M. Alpha-1 Antitrypsin Deficiency and COVID-19 Infection. Arch. Bronconeumol. 2020, 57, 97. [Google Scholar] [CrossRef] [PubMed]
- Wettstein, L.; Weil, T.; Conzelmann, C.; Müller, J.A.; Groß, R.; Hirschenberger, M.; Seidel, A.; Klute, S.; Zech, F.; Bozzo, C.P.; et al. Alpha-1 antitrypsin inhibits TMPRSS2 protease activity and SARS-CoV-2 infection. Nat. Commun. 2021, 12, 1726. [Google Scholar] [CrossRef]
- Ritzmann, F.; Chitirala, P.; Krüger, N.; Hoffmann, M.; Zuo, W.; Lammert, F.; Smola, S.; Tov, N.; Alagem, N.; Lepper, P.M.; et al. Therapeutic Application of Alpha-1 Antitrypsin in COVID-19. Am. J. Respir. Crit. Care Med. 2021, 204, 224–227. [Google Scholar] [CrossRef]
- Ritonavir-Boosted Nirmatrelvir (Paxlovid)|COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/antivirals-including-antibody-products/ritonavir-boosted-nirmatrelv-ir--paxlovid-/#:%E2%88%BC:text=Nirmatrelvir%20is%20an%20orally%20bioavailable,cleaving%20the%202%20viral%20polyproteins (accessed on 30 March 2023).
- Toussi, S.S.; Neutel, J.M.; Navarro, J.; Preston, R.A.; Shi, H.; Kavetska, O.; LaBadie, R.R.; Binks, M.; Chan, P.L.; Demers, N.; et al. Pharmacokinetics of Oral Nirmatrelvir/Ritonavir, a Protease Inhibitor for Treatment of COVID-19, in Subjects With Renal Impairment. Clin. Pharmacol. Ther. 2022, 112, 892–900. [Google Scholar] [CrossRef]
- Shinoda, R.; Shinoda, Y.; Ohashi, K.; Matsuoka, T.; Hirose, T.; Sugiyama, T.; Yoshimura, T. Single-centre retrospective observational study comparing trough blood concentration and safety of teicoplanin formulations. J. Infect. Chemother. 2019, 25, 563–566. [Google Scholar] [CrossRef]
- Abdulkarim, A.; Craig, T.J. Alpha 1 Antitrypsin Mutation; StatPearls: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Pasley, M.V.; Martínez, M.; Hermes, A.; d’Amico, R.; Nilius, A. Safety and Efficacy of Lopinavir/Ritonavir during Preg-nancy: A Systematic Review. AIDS Rev. 2013, 15, 38–48. [Google Scholar]
- Weiss, R.J.; Esko, J.D.; Tor, Y. Targeting heparin and heparan sulfate protein interactions. Org. Biomol. Chem. 2017, 15, 5656–5668. [Google Scholar] [CrossRef]
- Barrett, C.D.; Moore, H.B.; Yaffe, M.B.; Moore, E.E. ISTH interim guidance on recognition and management of coagulopathy in COVID-19: A comment. J. Thromb. Haemost. 2020, 18, 2060–2063. [Google Scholar] [CrossRef]
- Mangiafico, M.; Caff, A.; Costanzo, L. The Role of Heparin in COVID-19: An Update after Two Years of Pandemics. J. Clin. Med. 2022, 11, 3099. [Google Scholar] [CrossRef]
- Zhang, R.; Ni, L.; Di, X.; Wang, X.; Ma, B.; Niu, S.; Liu, C. Systematic review and meta-analysis of the prevalence of venous thromboembolic events in novel coronavirus disease-2019 patients. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 9, 289–298.e5. [Google Scholar] [CrossRef]
- Kollias, A.; Kyriakoulis, K.G.; Lagou, S.; Kontopantelis, E.; Stergiou, G.S.; Syrigos, K. Venous thromboembolism in COVID-19: A systematic review and meta-analysis. Vasc. Med. 2021, 26, 415–425. [Google Scholar] [CrossRef]
- Slobodnick, A.; Shah, B.; Krasnokutsky, S.; Pillinger, M.H. Update on colchicine, 2017. Rheumatology 2017, 57, i4–i11. [Google Scholar] [CrossRef] [PubMed]
- Leung, Y.Y.; Yao Hui, L.L.; Kraus, V.B. Colchicine—Update on mechanisms of action and therapeutic uses. Semin. Arthritis Rheum. 2015, 45, 341–350. [Google Scholar] [CrossRef]
- Reyes, A.Z.; A Hu, K.; Teperman, J.; Muskardin, T.L.W.; Tardif, J.-C.; Shah, B.; Pillinger, M.H. Anti-inflammatory therapy for COVID-19 infection: The case for colchicine. Ann. Rheum. Dis. 2020, 80, 550–557. [Google Scholar] [CrossRef]
- Burrage, D.R.; Koushesh, S.; Sofat, N. Immunomodulatory Drugs in the Management of SARS-CoV-2. Front. Immunol. 2020, 11, 1844. [Google Scholar] [CrossRef]
- Vaidya, K.; Arnott, C.; Martínez, G.J.; Ng, B.; McCormack, S.; Sullivan, D.R.; Celermajer, D.S.; Patel, S. Colchicine Therapy and Plaque Stabilization in Patients With Acute Coronary Syndrome: A CT Coronary Angiography Study. JACC Cardiovasc. Imaging 2017, 11, 305–316. [Google Scholar] [CrossRef]
- Demidowich, A.P.; CHI Consortium; Levine, J.A.; Apps, R.; Cheung, F.K.; Chen, J.; Fantoni, G.; Patel, T.P.; Yanovski, J.A. Colchicine’s effects on metabolic and inflammatory molecules in adults with obesity and metabolic syndrome: Results from a pilot randomized controlled trial. Int. J. Obes. 2020, 44, 1793–1799. [Google Scholar] [CrossRef]
- Schlesinger, N.; Firestein, B.L.; Brunetti, L. Colchicine in COVID-19: An Old Drug, New Use. Curr. Pharmacol. Rep. 2020, 6, 137–145. [Google Scholar] [CrossRef]
- Mikolajewska, A.; Fischer, A.L.; Piechotta, V.; Mueller, A.; Metzendorf, M.I.; Becker, M.; Dorando, E.; Pacheco, R.L.; Martim-bianco, A.L.C.; Riera, R.; et al. Colchicine for the Treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 2021, CD015045. [Google Scholar] [CrossRef]
- Absalón-Aguilar, A.; Rull-Gabayet, M.; Pérez-Fragoso, A.; Mejía-Domínguez, N.R.; Núñez-Álvarez, C.; Kershenobich-Stalnikowitz, D.; Sifuentes-Osornio, J.; Ponce-De-León, A.; González-Lara, F.; Martín-Nares, E.; et al. Colchicine Is Safe Though Ineffective in the Treatment of Severe COVID-19: A Randomized Clinical Trial (COLCHIVID). J. Gen. Intern. Med. 2021, 37, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Drug and Treatment Tracker—The New York Times. Available online: https://www.nytimes.com/interactive/2020/science/coronavirus-drugs-treatments.html (accessed on 30 March 2023).



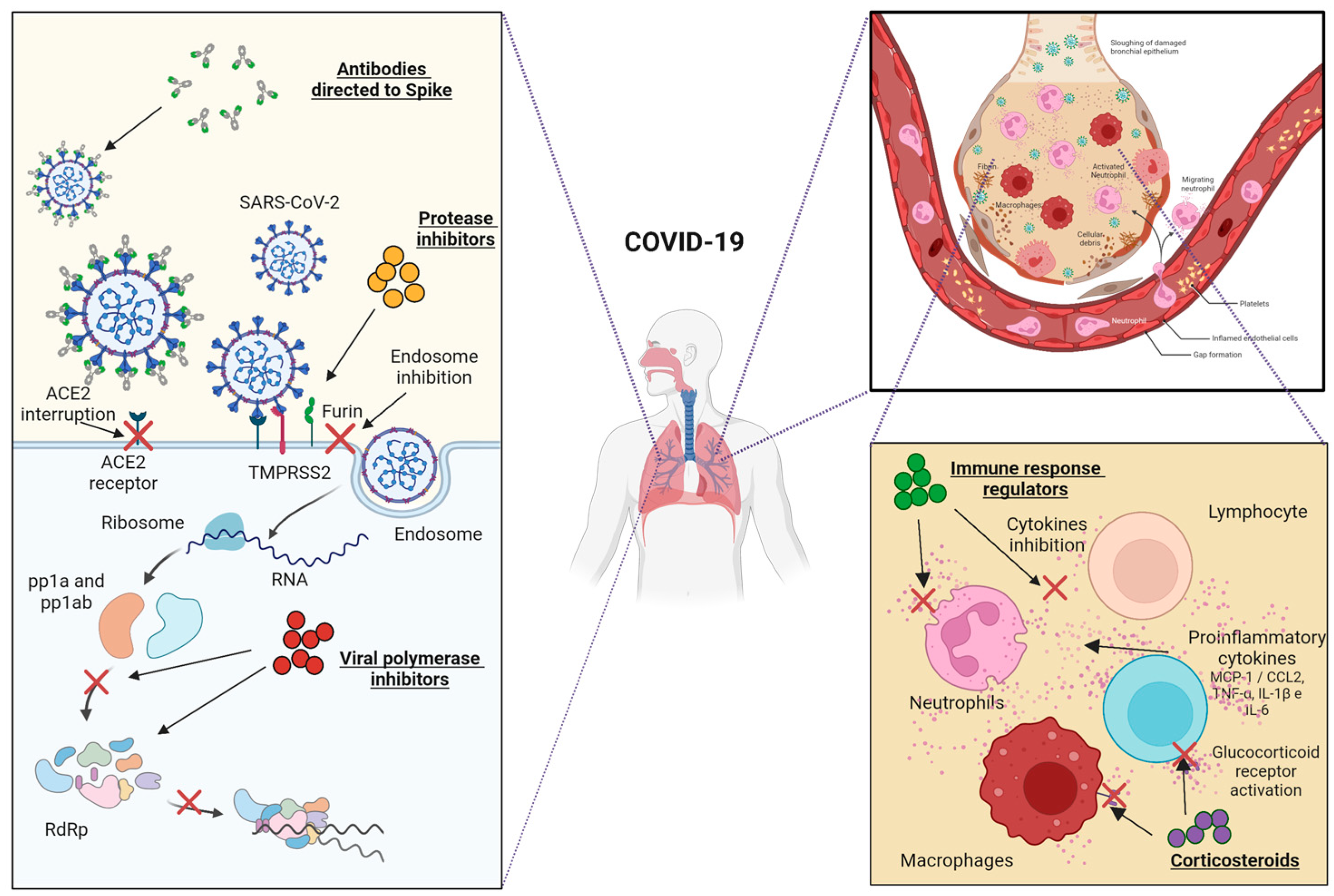{kind=link}
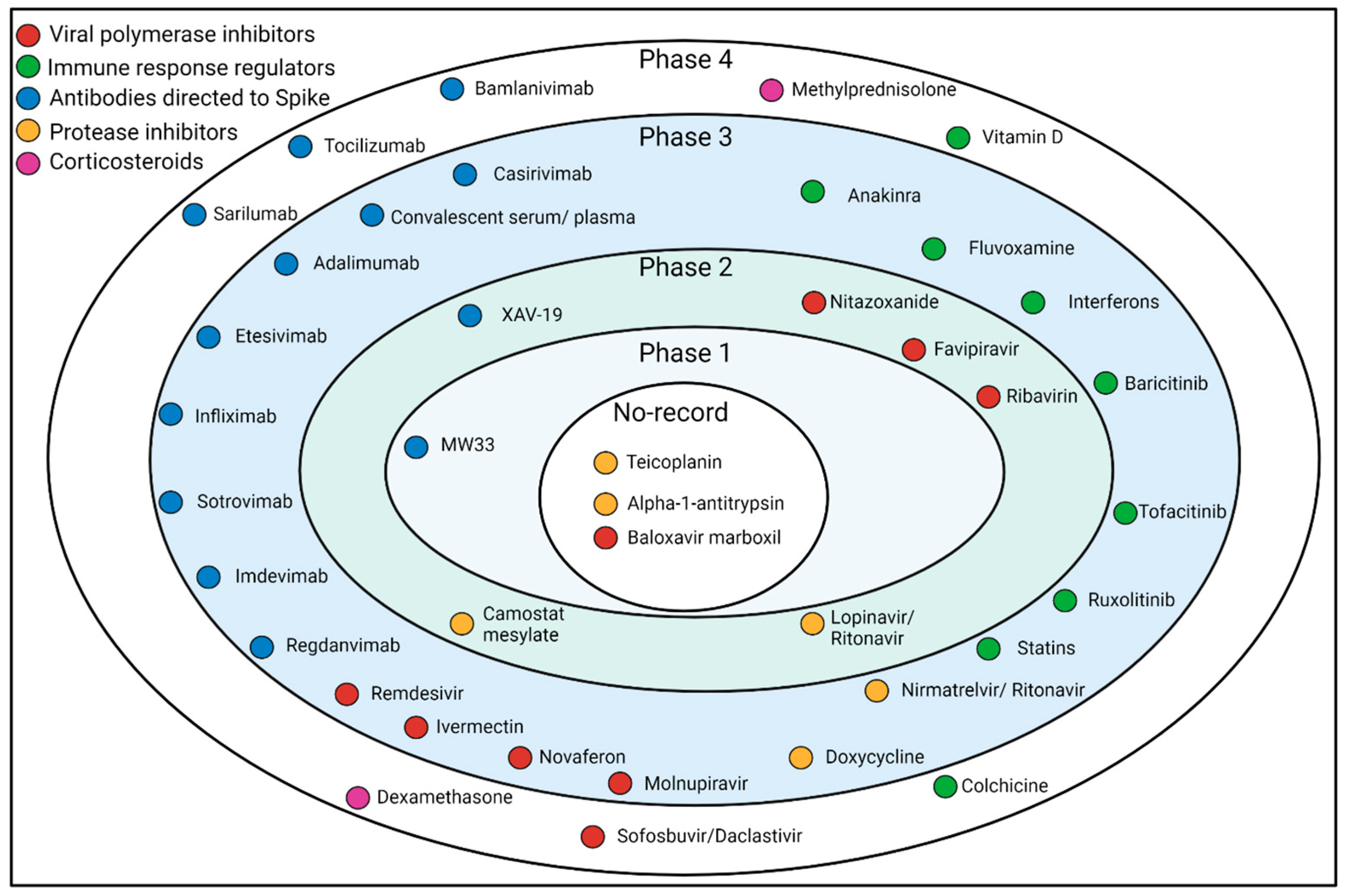{kind=link}
| mAbs | Source | Admin | Phase | Identification Register | Use | Main Sponsor | Cite |
|---|---|---|---|---|---|---|---|
| casirivimab and imdevimab | Recombinant Human/Humanized mice | Cocktail | 1/2/3 | NCT04425629 | Ambulatory | Regeneron, Greenburgh, NY, USA | [54] |
| casirivimab and imdevimab | Recombinant Human/Humanized mice | Cocktail | 1/2/3 | NCT04426695 | Hospitalized patients | Regeneron | [74] |
| casirivimab and imdevimab | Recombinant Human/Humanized mice | Cocktail | 3 | NCT04452318 | Prophylaxis | Regeneron | [75] |
| MW33 | Recombinant | Monotherapy | 1 | NCT04533048 | Ambulatory | Mabwell (Shanghai) Bioscience Co., Ltd., Shanghai, China | [76] |
| MW33 | Recombinant | Monotherapy | 2 | NCT04627584 | Ambulatory | Mabwell (Shanghai) Bioscience Co., Ltd. | [76] |
| BRII-196 and BRII-198 | Recombinant Human | Cocktail | 2/3 | NCT05780424 | Ambulatory | Eli Lilly, Indianapolis, IN, USA | [77] |
| BRII-196 | Recombinant Human | Monotherapy | 1 | NCT04479631 | Ambulatory | Brii Biosciences Limited, Beijing, China | [18] |
| BRII-198 | Recombinant Human | Monotherapy | 1 | NCT04479644 | Ambulatory | Brii Biosciences Limited | [18] |
| AZD8895 and AZD1061 | Recombinant Human | Cocktail | 3 | NCT04625725 | Ambulatory | AstraZeneca, Cambridge, UK | [78] |
| XAV-19 | Polyclonal Humanized | Monotherapy | 2 | NCT04453384 | Hospitalized patients | Nantes University Hospital, Nantes, France | [79] |
| XAV-19 | Polyclonal Humanized | Monotherapy | 2/3 | NCT04928430 | Hospitalized patients | Xenothera SAS, Nantes, France | [79] |
| Sotrovimab | Recombinant Human | Monotherapy | 1 | NCT04988152 | Ambulatory | Vir Biotechnology, Inc., San Francisco, CA, USA | [80] |
| Sotrovimab | Recombinant Human | Monotherapy | 2/3 | NCT04545060 | Ambulatory | Vir Biotechnology, Inc. | [81] |
| Regdanvimab | Recombinant Human | Monotherapy | 1 | NCT04593641 | Ambulatory | Celltrion, Incheon, Republic of Korea | [82] |
| Regdanvimab | Recombinant Human | Monotherapy | 2/3 | NCT04602000 | Ambulatory | Celltrion | [82] |
| Drug | Doses | Comparator | Phase | Identification Register | Use | Main Sponsor | Cite |
|---|---|---|---|---|---|---|---|
| Remdesivir | One dose of 200 mg on day 1, followed by doses of 100 mg iv once a day for nine days | Remdesivir placebo | 3 | NCT04257656 | Hospitalized Patients | China-Japan Friendship Hospital | [212] |
| Ribavirin | Oral Lopinavir/ritonavir: 400 mg/100 mg twice daily for 14 days; oral Ribavirin 400 mg twice daily for 14 days; Interferon Beta-1B 0.25 mg subcutaneous injection alternate days for three days | Lopinavir/ritonavir | 2 | NCT04276688 | Hospitalized Patients | The University of Hong Kong | [213] |
| Favipiravir | Oral avipiravir 1600 mg stat and then 600 mg every 8 h plus hydroxychloroquine 200 mg twice a day for 1 week | Lopinavir/Ritonavir and hydroxychloroquine | 3 | IRCT20151227025726N14 | Patients with moderate to severe COVID-19 | Royal College of Surgeons in Ireland—Medical University of Bahrain | [214] |
| Molnupiravir | Oral doses of 200/400/800 mg every 12 h for five days | Placebo | 2/3 | NCT04575584 | Hospitalized Patients | Merck Sharp and Dohme Corp | [215] |
| Sofosbuvir/ Daclastavir | Oral Sofosbuvir 400 mg plus Daclatasvir 200 mg for day | Standard clinical care | 3 | NCT04535869 | Patients with Moderate to severe COVID-19 | Mansoura University | [216] |
| Drug | Doses | Comparator | Phase | Identification Register | Use | Main Sponsor | Cite |
|---|---|---|---|---|---|---|---|
| Dexamethasone | 20 mg/iv/daily/from Day 1 of randomization during 5 days, followed by 10 mg/iv/daily from Day 6 to 10 of randomization | Standard clinical care | 4 | NCT04325061 | Patients intubated and mechanically ventilated | Dr. Negrin University Hospital | [253] |
| Methylprednisolone | 1 mg/kg/day given intravenously for five days | Dexamethasone | 3 | NCT04603729 | Patients with moderate to severe COVID-19 | Fatima Memorial Hospital | [254] |
| Drug | Doses | Comparator | Phase | Identification Register | Use | Main Sponsor | Cite |
|---|---|---|---|---|---|---|---|
| Nirmatrelvir/ Ritonavir | 300/100 mg every 12 h for 5 days | Placebo | 3 | NCT04960202 | Ambulatory | Pfizer | [275] |
| Lopinavir/ Ritonavir | 200 mg/100 mg 2 tablets by mouth, every 12 h for 7–10 days | Hydroxychloroquine | 2 | NCT04307693 | Ambulatory | Asan Medical Center | [276] |
| Camostat mesylate | 200 mg taken orally, four times daily, for seven days | Placebo | 2 | NCT04353284 | Ambulatory | Yale University | [277] |
| Alpha-1-antitrypsin | Administration based on clinical indication | No comparator | No records | NCT04799873 | Patients without the need for invasive ventilation | Universität des Saarlandes | [278] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceja-Gálvez, H.R.; Renteria-Flores, F.I.; Nicoletti, F.; Hernández-Bello, J.; Macedo-Ojeda, G.; Muñoz-Valle, J.F. Severe COVID-19: Drugs and Clinical Trials. J. Clin. Med. 2023, 12, 2893. https://doi.org/10.3390/jcm12082893
Ceja-Gálvez HR, Renteria-Flores FI, Nicoletti F, Hernández-Bello J, Macedo-Ojeda G, Muñoz-Valle JF. Severe COVID-19: Drugs and Clinical Trials. Journal of Clinical Medicine. 2023; 12(8):2893. https://doi.org/10.3390/jcm12082893
Chicago/Turabian StyleCeja-Gálvez, Hazael Ramiro, Francisco Israel Renteria-Flores, Ferdinando Nicoletti, Jorge Hernández-Bello, Gabriela Macedo-Ojeda, and José Francisco Muñoz-Valle. 2023. "Severe COVID-19: Drugs and Clinical Trials" Journal of Clinical Medicine 12, no. 8: 2893. https://doi.org/10.3390/jcm12082893