
Common Data Elements Reported in Mechanical Thrombectomy for Acute Ischemic Stroke: A Systematic Review of Active Clinical Trials
 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Literature Search and Study Selection
2.2. Tagging and Common Data Elements
2.3. Data Synthesis
3. Results
3.1. Semi-Automated Search Results
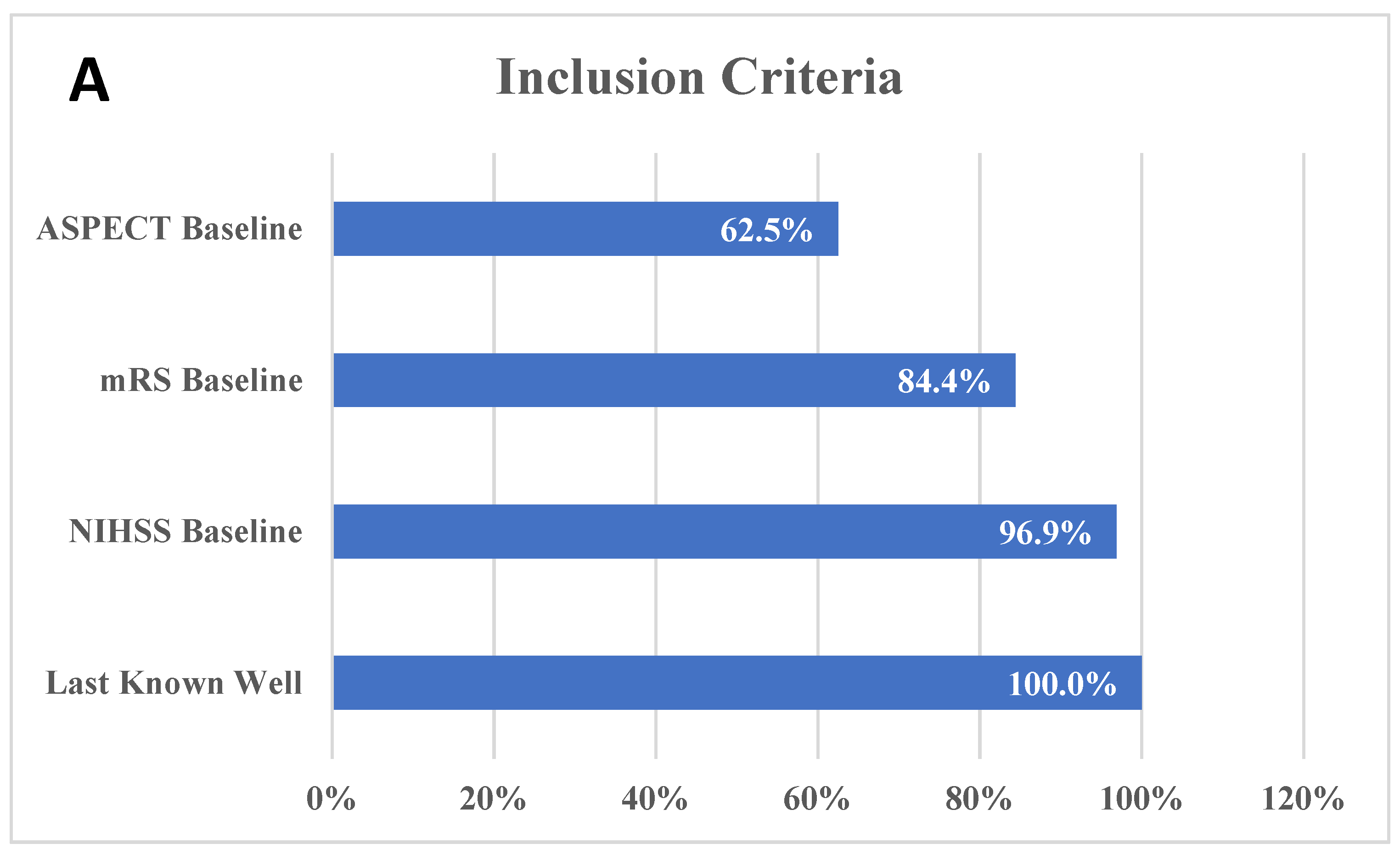
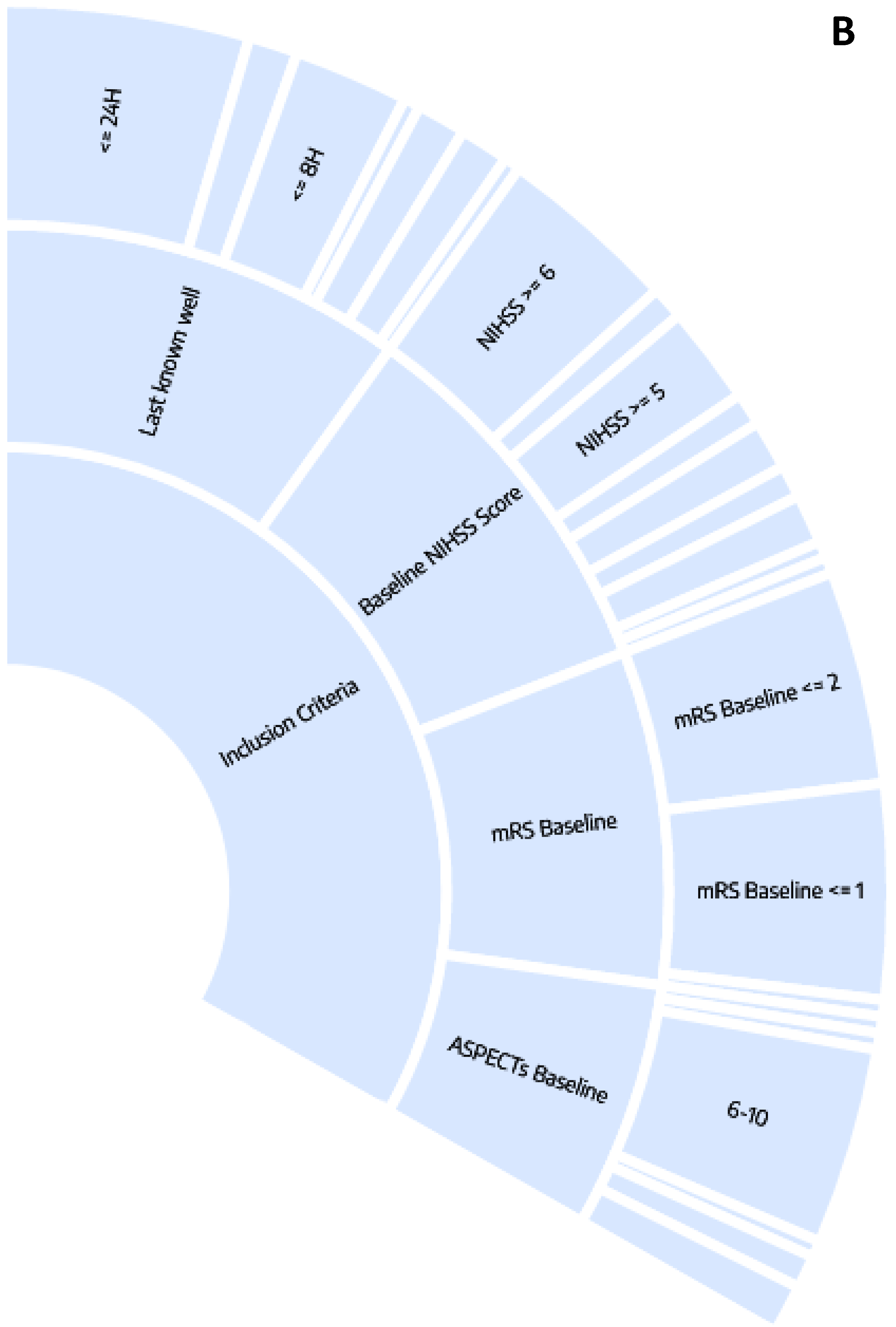
3.2. Inclusion Criteria
3.3. Interventions
3.4. Reported Outcomes
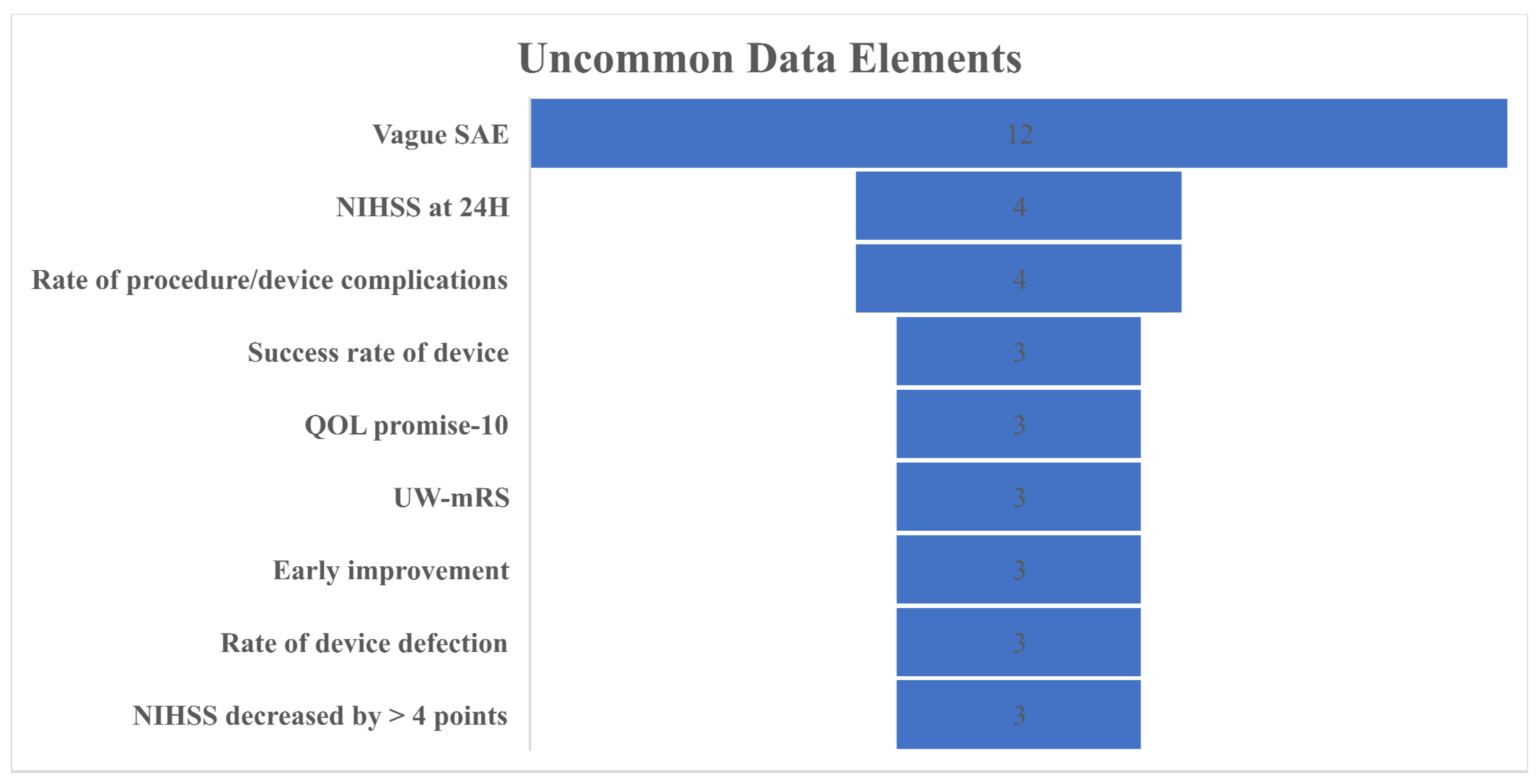
3.5. Uncommon Data Elements
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N. Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, P.S.; Butt, W.; Podlasek, A.; McConachie, N.; Lenthall, R.; Nair, S.; Malik, L.; Bhogal, P.; Makalanda, H.L.D.; Spooner, O.; et al. Association between time to treatment and clinical outcomes in endovascular thrombectomy beyond 6 hours without advanced imaging selection. J. Neurointerv. Surg. 2022. [Google Scholar] [CrossRef]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; de Miquel, M.A.; Molina, C.A.; Rovira, A.; San Román, L.; Serena, J.; Abilleira, S.; Ribó, M.; et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef] [Green Version]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Correction to: Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e440–e441. [Google Scholar]
- Bhogal, P.; Andersson, T.; Maus, V.; Mpotsaris, A.; Yeo, L. Mechanical Thrombectomy-A Brief Review of a Revolutionary new Treatment for Thromboembolic Stroke. Clin. Neuroradiol. 2018, 28, 313–326. [Google Scholar] [CrossRef]
- Li, C.; Wu, C.; Wu, L.; Zhao, W.; Chen, J.; Ren, M.; Yao, C.; Yan, X.; Dong, C.; Song, H.; et al. Basilar Artery Occlusion Chinese Endovascular Trial: Protocol for a prospective randomized controlled study. Int. J. Stroke 2021, 2021, 17474930211040923. [Google Scholar] [CrossRef] [PubMed]
- Tao, C.; Li, R.; Zhu, Y.; Qun, S.; Xu, P.; Wang, L.; Zhang, C.; Liu, T.; Song, J.; Sun, W.; et al. Endovascular treatment for acute basilar artery occlusion: A multicenter randomized controlled trial (ATTENTION). Int. J. Stroke 2022, 2022, 17474930221077164. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Adusumilli, G.; Ghozy, S.; Kallmes, K.M.; Hardy, N.; Tarchand, R.; Zinn, C.; Lamar, D.; Singeltary, E.; Siegel, L.; Kallmes, D.F.; et al. Common data elements reported on middle meningeal artery embolization in chronic subdural hematoma: An interactive systematic review of recent trials. J. Neurointerv. Surg. 2022, 14, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Dastgir, J.; Rutkowski, A.; Alvarez, R.; Cossette, S.A.; Yan, K.; Hoffmann, R.G.; Sewry, C.; Hayashi, Y.K.; Goebel, H.H.; Bonnemann, C.; et al. Common Data Elements for Muscle Biopsy Reporting. Arch. Pathol. Lab. Med. 2016, 140, 51–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadkarni, P.M.; Brandt, C.A. The Common Data Elements for cancer research: Remarks on functions and structure. Methods Inf. Med. 2006, 45, 594–601. [Google Scholar] [PubMed] [Green Version]
- Redeker, N.S.; Anderson, R.; Bakken, S.; Corwin, E.; Docherty, S.; Dorsey, S.G.; Heitkemper, M.; McCloskey, D.J.; Moore, S.; Pullen, C.; et al. Advancing Symptom Science Through Use of Common Data Elements. J. Nurs. Scholarsh. 2015, 47, 379–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saver, J.L.; Warach, S.; Janis, S.; Odenkirchen, J.; Becker, K.; Benavente, O.; Broderick, J.; Dromerick, A.W.; Duncan, P.; Elkind, M.S.; et al. Standardizing the structure of stroke clinical and epidemiologic research data: The National Institute of Neurological Disorders and Stroke (NINDS) Stroke Common Data Element (CDE) project. Stroke 2012, 43, 967–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taruscio, D.; Mollo, E.; Gainotti, S.; Posada de la Paz, M.; Bianchi, F.; Vittozzi, L. The EPIRARE proposal of a set of indicators and common data elements for the European platform for rare disease registration. Arch. Public Health 2014, 72, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, E.; Kang, H. Introduction to systematic review and meta-analysis. Korean, J. Anesthesiol. 2018, 71, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montori, V.M.; Swiontkowski, M.F.; Cook, D.J. Methodologic issues in systematic reviews and meta-analyses. Clin. Orthop. Relat. Res. 2003, 413, 43–54. [Google Scholar] [CrossRef]
- Uman, L.S. Systematic reviews and meta-analyses. J. Can. Acad. Child Adolesc. Psychiatry 2011, 20, 57–59. [Google Scholar]
- Ren, Z.; Huo, X.; Ma, G.; Tong, X.; Kumar, J.; Pressman, E.; Chen, W.; Yuan, G.; Wang, A.Y.; Wei, M.; et al. Selection criteria for large core trials: Rationale for the ANGEL-ASPECT study design. J. Neurointerv. Surg. 2022, 14, 107–110. [Google Scholar] [CrossRef]
- Azzam, A.Y.; Ghozy, S.; Kallmes, K.M.; Adusumilli, G.; Heit, J.J.; Hassan, A.E.; Kadirvel, R.; Kallmes, D.F. Aspiration thrombectomy versus stent retriever thrombectomy alone for acute ischemic stroke: Evaluating the overlapping meta-analyses. J. Neurointerv. Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Saber, H.; Rajah, G.B.; Kherallah, R.Y.; Jadhav, A.P.; Narayanan, S. Comparison of the efficacy and safety of thrombectomy devices in acute stroke: A network meta-analysis of randomized trials. J. Neurointerv. Surg. 2018, 10, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Qiu, S.; Wang, L.; Li, Y.; Wang, D.; Liu, M. Comparison of Four Food and Drug Administration-Approved Mechanical Thrombectomy Devices for Acute Ischemic Stroke: A Network Meta-Analysis. World Neurosurg. 2019, 127, e49–e57. [Google Scholar] [CrossRef] [PubMed]
- Ghozy, S.; Kacimi, S.E.O.; Azzam, A.Y.; Farahat, R.A.; Abdelaal, A.; Kallmes, K.M.; Adusumilli, G.; Heit, J.J.; Kadirvel, R.; Kallmes, D.F. Successful mechanical thrombectomy in acute ischemic stroke: Revascularization grade and functional independence. J. Neurointerv. Surg. 2022, 14, 779–782. [Google Scholar] [CrossRef]
- Kaesmacher, J.; Dobrocky, T.; Heldner, M.R.; Bellwald, S.; Mosimann, P.J.; Mordasini, P.; Bigi, S.; Arnold, M.; Gralla, J.; Fischer, U. Systematic review and meta-analysis on outcome differences among patients with TICI2b versus TICI3 reperfusions: Success revisited. J. Neurol. Neurosurg. Psychiatry 2018, 89, 910–917. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, A.; Seyedsaadat, S.M.; Murad, M.H.; Brinjikji, W.; Fitzgerald, S.T.; Kadirvel, R.; Rabinstein, A.A.; Kallmes, D.F. Redefining ‘success’: A systematic review and meta-analysis comparing outcomes between incomplete and complete revascularization. J. Neurointerv. Surg. 2019, 11, 9–13. [Google Scholar] [CrossRef]
- Langezaal, L.C.M.; van der Hoeven, E.; Mont’Alverne, F.J.A.; de Carvalho, J.J.F.; Lima, F.O.; Dippel, D.W.J.; van der Lugt, A.; Lo, R.T.H.; Boiten, J.; Lycklama, À. Nijeholt, G.J.; et al. Endovascular Therapy for Stroke Due to Basilar-Artery Occlusion. N. Engl. J. Med. 2021, 384, 1910–1920. [Google Scholar] [CrossRef]
- Yoshimura, S.; Sakai, N.; Yamagami, H.; Uchida, K.; Beppu, M.; Toyoda, K.; Matsumaru, Y.; Matsumoto, Y.; Kimura, K.; Takeuchi, M.; et al. Endovascular Therapy for Acute Stroke with a Large Ischemic Region. N. Engl. J. Med. 2022, 386, 1303–1313. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghozy, S.; Hardy, N.; Sutphin, D.J.; Kallmes, K.M.; Kadirvel, R.; Kallmes, D.F. Common Data Elements Reported in Mechanical Thrombectomy for Acute Ischemic Stroke: A Systematic Review of Active Clinical Trials. Brain Sci. 2022, 12, 1679. https://doi.org/10.3390/brainsci12121679
Ghozy S, Hardy N, Sutphin DJ, Kallmes KM, Kadirvel R, Kallmes DF. Common Data Elements Reported in Mechanical Thrombectomy for Acute Ischemic Stroke: A Systematic Review of Active Clinical Trials. Brain Sciences. 2022; 12(12):1679. https://doi.org/10.3390/brainsci12121679
Chicago/Turabian StyleGhozy, Sherief, Nicole Hardy, Daniel J. Sutphin, Kevin M. Kallmes, Ramanathan Kadirvel, and David F. Kallmes. 2022. "Common Data Elements Reported in Mechanical Thrombectomy for Acute Ischemic Stroke: A Systematic Review of Active Clinical Trials" Brain Sciences 12, no. 12: 1679. https://doi.org/10.3390/brainsci12121679