
A Study of the Epidemiology, Clinical, and Phenotypic Characteristics of Inflammatory Bowel Disease in the Northen-Central Region of Saudi Arabia

 and
and
Abstract
:1. Introduction
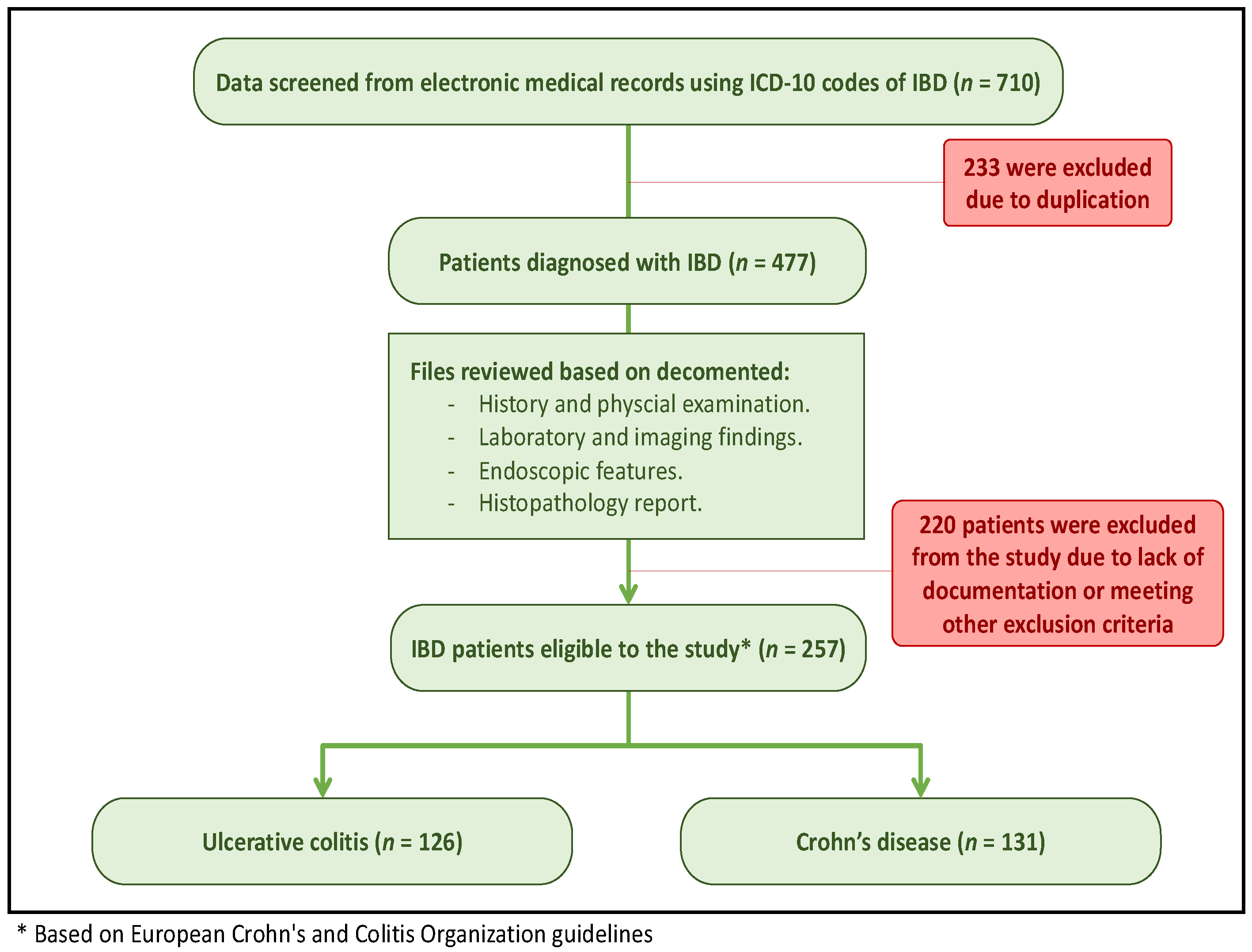
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Collection Methods
2.3. Study Sample
2.4. Quality Assessment
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Orholm, M.; Munkholm, P.; Langholz, E.; Nielsen, O.H.; Sørensen, T.I.; Binder, V. Familial occurrence of inflammatory bowel disease. N. Engl. J. Med. 1991, 324, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Danese, S.; Sans, M.; Fiocchi, C. Inflammatory bowel disease: The role of environmental factors. Autoimmun. Rev. 2004, 3, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, D.C.; Carding, S.R. Inflammatory bowel disease: Cause and immunobiology. Lancet 2007, 369, 1627–1640. [Google Scholar] [CrossRef] [PubMed]
- Molodecky, N.A.; Soon, I.S.; Rabi, D.M.; Ghali, W.A.; Ferris, M.; Chernoff, G.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Barkema, H.W.; et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 2012, 142, 46–54.e42. [Google Scholar] [CrossRef] [Green Version]
- Loftus, E.V. Clinical epidemiology of inflammatory bowel disease: Incidence, prevalence, and environmental influences. Gastroenterology 2004, 126, 1504–1517. [Google Scholar] [CrossRef]
- Kirsner, J.B.; Shorter, R.G. Recent developments in nonspecific inflammatory bowel disease (second of two parts). N. Engl. J. Med. 1982, 306, 837–848. [Google Scholar] [CrossRef]
- Burisch, J.; Pedersen, N.; Cukovic-Cavka, S.; Brinar, M.; Kaimakliotis, I.; Duricova, D.; Shonová, O.; Vind, I.; Avnstrøm, S.; Thorsgaard, N.; et al. East-West gradient in the incidence of inflflammatory bowel disease in Europe: The ECCO-EpiCom inception cohort. Gut 2014, 63, 588–597. [Google Scholar] [CrossRef]
- María, C.; Garre, A.; Ortiz, A.N.; Palomares, M.T.D.-L.; GETECCU. Incidence, Clinical Characteristics and Management of Inflammatory Bowel Disease in Spain: Large-Scale Epidemiological Study. J. Clin. Med. 2021, 10, 2885. [Google Scholar] [CrossRef]
- Al-Ghamdi, A.S.; Al-Mofleh, I.A.; Al-Rashed, R.S.; Al-Amri, S.M.; Aljebreen, A.M.; Isnani, A.C.; El-Badawi, R. Epidemiology and outcome of Crohn’s disease in a teaching hospital in Riyadh. World J. Gastroenterol. 2004, 10, 1341–1344. [Google Scholar] [CrossRef]
- El-Sheikh, M.A.; Al Karawi, M.A.; Hamid, M.A.; Yasawy, I. Lower gastrointestinal tract pathology in Saudis: Results of endoscopic biopsy findings in 1600 patients. Ann. Saudi Med. 1987, 7, 306–311. [Google Scholar] [CrossRef]
- Hossain, J.; Al-Mofleh, I.A.; Laajam, M.A.; Al-Rashed, R.S.; Al-Faleh, F.Z. Crohn’s disease in Arabs. Ann. Saudi Med. 1991, 11, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Hossain, J.; Al-Faleh, F.Z.; Al-Mofleh, I.; Al-Aska, A.; Laajam, M.A.; Al-Rashed, R. Does ulcerative colitis exist in Saudi Arabia? Analysis of thirty-seven cases. Saudi Med. J. 1989, 10, 360–362. [Google Scholar]
- Khan, H.A.; Mahrous, A.S.; Khawaja, F.L. Ulcerative colitis among the Saudis: Six year experience from Al-Madinah region. Saudi J. Gastroenterol. 1996, 2, 69–73. [Google Scholar] [PubMed]
- Contractor, Q.Q.; Contractor, T.Q.; Ul Haque, I.; El Mahdi El Mel, B. Ulcerative colitis: Al-gassim experience. Saudi J. Gastroenterol. 2004, 10, 22–27. [Google Scholar] [PubMed]
- Contractor, Q.Q.; Contractor, T.Q.; Ul Haque, I.; El Mahdi El Mel, B. Crohn’s disease among Saudis in Al-Gassim region. Saudi J. Gastroenterol. 2005, 11, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Al-Mofarreh, M.A.; Al-Mofleh, I.A. Emerging inflammatory bowel disease in Saudi outpatients: A report of 693 cases. Saudi J. Gastroenterol. 2013, 19, 16–22. [Google Scholar] [CrossRef]
- Al Fadda, M.; Peedikayil, M.C.; Kagevi, I.; Al Kahtani, K.; Al Ben Mousa, A.; Al Ashgar, H.I.; Al Sohaibani, F.; Al Quaiz, M.; Abdulla, M.; Khan, M.Q.; et al. Inflammatory bowel disease in Saudi Arabia: A hospital-based clinical study of 312 patients. Ann. Saudi Med. 2012, 32, 276–282. [Google Scholar] [CrossRef] [Green Version]
- Kappelman, M.D.; Rifas-Shiman, S.L.; Kleinman, K.; Ollendorf, D.; Bousvaros, A.; Grand, R.J.; Finkelstein, J.A. The prevalence and geographic distribution of Crohn’s disease and ulcerative colitis in the United States. Clin. Gastroenterol. Hepatol. 2007, 5, 1424–1429. [Google Scholar] [CrossRef]
- Shivashankar, R.; Tremaine, W.J.; Harmsen, W.S.; Loftus, E.V. Incidence and prevalence of Crohn’s disease and ulcerative colitis in Olmsted County, Minnesota from 1970 through. Clin. Gastroenterol. Hepatol. 2017, 15, 857–863. [Google Scholar] [CrossRef]
- Siddique, I.; Alazmi, W.; Al-Ali, J.; Al-Fadli, A.; Alateeqi, N.; Memon, A.; Hasan, F. Clinical epidemiology of Crohn’s disease in Arabs based on the Montreal classification. Inflamm. Bowel Dis. 2012, 18, 1689–1697. [Google Scholar] [CrossRef]
- Esmat, S.; El Nady, M.; Elfekki, M.; Elsherif, Y.; Naga, M. Epidemiological and clinical characteristics of inflammatory bowel diseases in Cairo, Egypt. World J. Gastroenterol. 2014, 20, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Mosli, M.; Alawadhi, S.; Hasan, F.; Abou Rached, A.; Sanai, F.; Danese, S. Incidence, Prevalence, and Clinical Epidemiology of Inflammatory Bowel Disease in the Arab World: A Systematic Review and Meta-Analysis. Inflamm. Intest. Dis. 2021, 6, 123–131. [Google Scholar] [CrossRef] [PubMed]
- The General Authority for Statistics (GAStat). Population Characteristics Survey 2017 A.D. Available online: https://www.stats.gov.sa/en/5725 (accessed on 17 June 2023).
- Munkholm, P.; Langholz, E.; Nielsen, O.H.; Kreiner, S.; Binder, V. Incidence and prevalence of Crohn’s disease in the county of Copenhagen, 1962–1987: A sixfold increase in incidence. Scand. J. Gastroenterol. 1992, 27, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Loftus, E.V.; Silverstein, M.D.; Sandborn, W.J.; Tremaine, W.J.; Harmsen, W.S.; Zinsmeister, A.R. Ulcerative colitis in Olmsted County, Minnesota, 1940–1993: Incidence, prevalence, and survival. Gut 2000, 46, 336–343. [Google Scholar] [CrossRef] [Green Version]
- Loftus, E.V., Jr.; Silverstein, M.D.; Sandborn, W.J.; Tremaine, W.J.; Harmsen, W.S.; Zinsmeister, A.R. Crohn’s disease in Olmsted County, Minnesota, 1940–1993: Incidence, prevalence, and survival. Gastroenterology 1998, 114, 1161–1168. [Google Scholar] [CrossRef]
- Henriksen, M.; Jahnsen, J.; Lygren, I.; Aadland, E.; Schulz, T.; Vatn, M.H.; Moum, B.; Ibsen Study Group. Clinical course in Crohn’s disease: Results of a five-year population-based follow-up study (the IBSEN study). Scand. J. Gastroenterol. 2007, 42, 602–610. [Google Scholar] [CrossRef]
- Aljebreen, A.M.; Alharbi, O.R.; Azzam, N.A.; Almalki, A.S.; Alswat, K.A.; Almadi, M.A. Clinical epidemiology and phenotypic characteristics of Crohn’s disease in the central region of Saudi Arabia. Saudi. J. Gastroenterol. 2014, 20, 162–169. [Google Scholar] [CrossRef]
- Adam, H.; Alqassas, M.; Saadah, O.I.; Mosli, M. Extraintestinal manifestations of inflammatory bowel disease in middle eastern patients. J. Epidemiol. Glob. Health. 2020, 10, 298–303. [Google Scholar] [CrossRef] [Green Version]
- Saleh, T.; Matta, F.; Yaekoub, A.Y.; Danescu, S.; Stein, P.D. Risk of venous thromboembolism with Inflammatory bowel disease. Clin. Appl. Thromb. Hemost 2011, 17, 254–258. [Google Scholar] [CrossRef]
- Gollop, J.H.; Phillips, S.F.; Melton, L.J., III; Zinsmeister, A.R. Epidemiologic Aspects of. Crohn’s disease: A population based study in Olmsted County, Minnesota, 1943–1982. Gut 1988, 29, 49–56. [Google Scholar] [CrossRef] [Green Version]
- Vermeire, S.; Van Assche, G.; Rutgeerts, P. Perianal Crohn’s Disease: Classification and clinical evaluation. Dig. Liver Dis. 2007, 39, 959–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellers, G.; Bergstrand, O.; Ewerth, S.; Holmstrom, B. Occurrence and outcome after primary treatment of anal fistulae in Crohn’s disease. Gut 1980, 21, 525–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, D.A.; Loftus, E.V.; Tremaine, W.J.; Panaccione, R.; Harmsen, W.S.; Zinsmeister, A.R.; Sandborn, W.J. The natural history of fistulizing Crohn’s disease in Olmsted County, Minnesota. Gastroenterology 2002, 122, 875–880. [Google Scholar] [CrossRef]
- Rankin, G.B.; Watts, H.; Melnyk, C.S.; Kelley, M.L. National Cooperative Crohn’s Disease Study: Extraintestinal manifestations and perianal complications. Gastroenterology 1979, 77, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Monsén, U.; Sorstad, J.; Hellers, G.; Johansson, C. Extracolonic diagnoses in ulcerative colitis: An epidemiological study. Am. J. Gastroenterol. 1990, 85, 711–716. [Google Scholar]
- Peyrin-Biroulet, L.; Loftus, E.V., Jr.; Colombel, J.F.; Sandborn, W.J. The natural history of adult Crohn’s disease in population-based cohorts. Am. J. Gastroenterol. 2010, 105, 289–297. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Overall n = 257 (100%) | UC n = 126 (49%) | CD n = 131 (51%) | p-Value | |
|---|---|---|---|---|---|
| Demographics | |||||
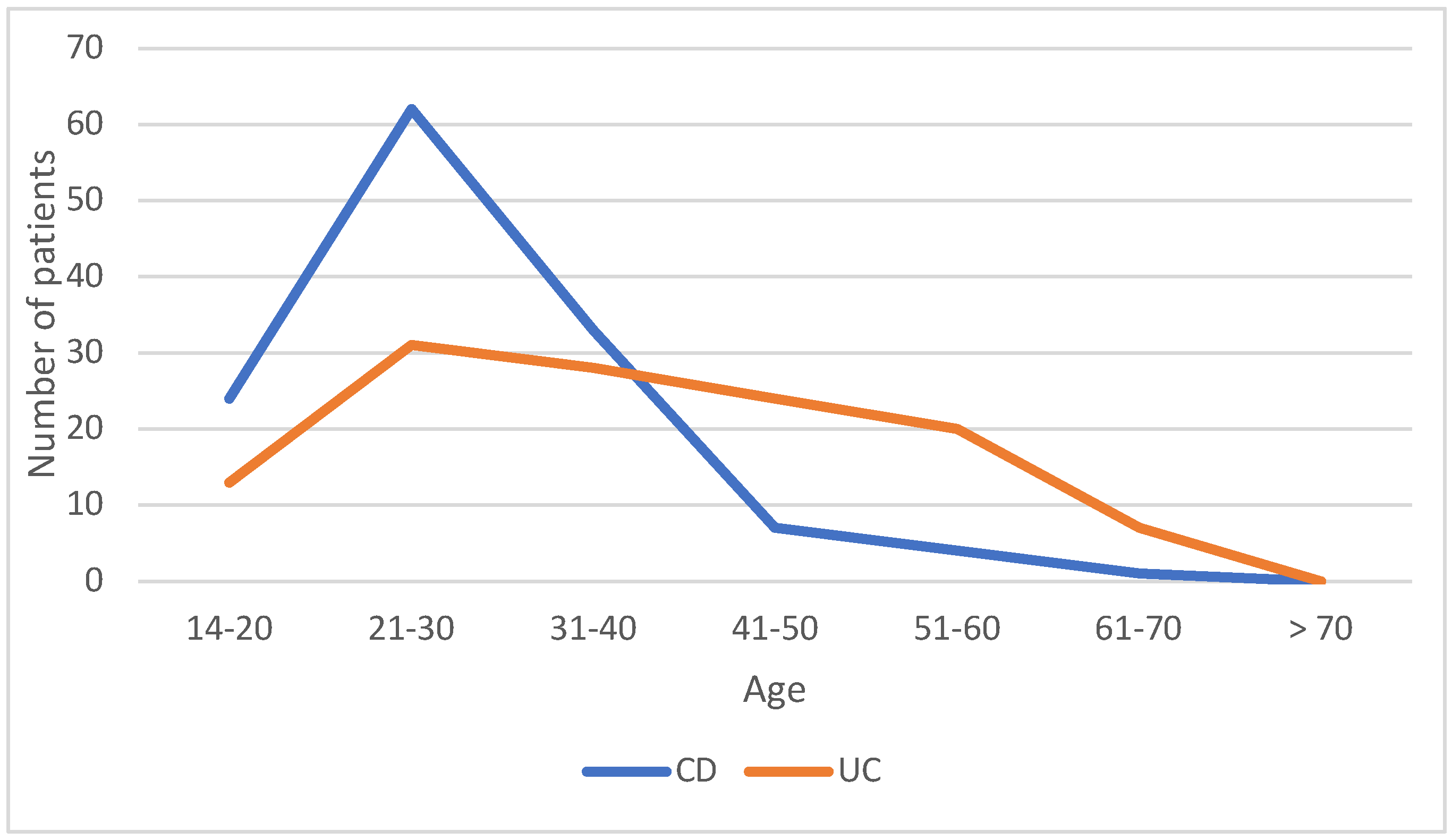
| Mean age (SD), years | 33.6 | 38.79 (14.9) | 28.74 (9.16) | ||
| <17 | 7 (2.7%) | 4 (3.2%) | 3 (2.3%) | 41.48 | <0.005 |
| 17–40 | 185 (71.9%) | 68 (53.9%) | 117 (89.3%) | ||
| >40 | 65 (25.2%) | 54 (42.8%) | 11 (8.4%) | ||
| Gender | |||||
| Male | 134 (52.1%) | 66 (52.4%) | 68 (52%) | 0.005 | 0.939 |
| Female | 123 (47.8%) | 60 (47.6%) | 63 (48%) | ||
| Extent of UC | |||||
| E1, n (%) | --- | 34 (27%) | --- | ||
| E2, n (%) | --- | 60 (47.6%) | --- | ||
| E3, n (%) | --- | 32 (25.4%) | --- | ||
| Age at CD diagnosis | |||||
| A1, n (%) | --- | --- | 17 (13%) | ||
| A2, n (%) | --- | --- | 107 (81.6%) | ||
| A3, n (%) | --- | --- | 7 (5.3%) | ||
| CD location | |||||
| L1, n (%) | --- | --- | 34 (26%) | ||
| L2, n (%) | --- | --- | 19 (14.5%) | ||
| L3, n (%) | --- | --- | 76 (58%) | ||
| L4, n (%) | --- | --- | 2 (1.5%) | ||
| CD behavior | |||||
| B1, n (%) | --- | --- | 70 (53.4%) | ||
| B2, n (%) | --- | --- | 32 (24.4%) | ||
| B3, n (%) | --- | --- | 29 (22.2%) | ||
| Perianal disease | |||||
| All, n (%) | 70 (27.2%) | 11 (8.7%) | 59 (45%) | 42.72 | <0.005 |
| Fistula, n (%) | 43 (16.7%) | 3 (2.3%) | 40 (30.5%) | 6.4259 | 0.011 |
| Fissure, n (%) | 14 (5.4%) | 5 (3.9%) | 9 (6.8%) | 5.285 | 0.021 |
| Abscess, n (%) | 13 (5%) | 3 (2.3%) | 10 (7.6%) | 0.653 | 0.418 |
| Extraintestinal manifestation | |||||
| All, n (%) | 45 (17.5%) | 19 (17.4%) | 26 (23.6%) | 1.010 | 0.314 |
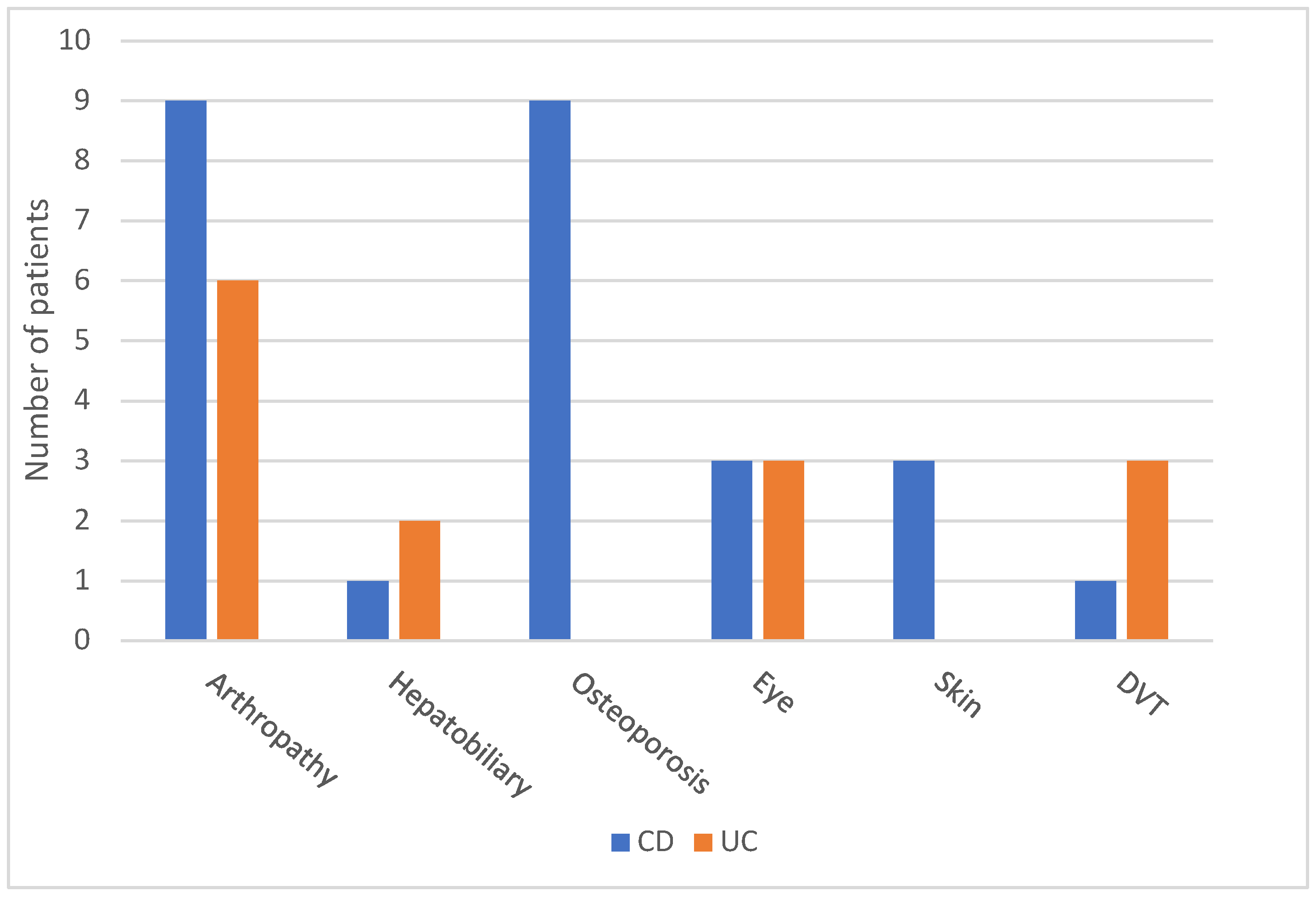
| Eye, n (%) | 6 (2.3%) | 3 (2.3%) | 3 (2.3%) | 0.200 | 0.653 |
| Skin, n (%) | 3 (1.1%) | 0 (0%) | 3 (2.3%) | 0.546 | 0.459 |
| Arthropathy | |||||
| Peripheral arthritis, n (%) | 8 (3.1%) | 6 (4.7%) | 2 (1.5%) | 4.352 | 0.036 |
| Sacroiliitis, n (%) | 7 (2.7%) | 0 (0%) | 7 (5.3%) | 3.265 | 0.070 |
| Hepatobiliary | |||||
| PSC, n (%) | 3 (1.1%) | 2 (1.5%) | 1 (0.8%) | 0.828 | 0.362 |
| Thromboembolic, n (%) | 4 (1.5%) | 3 (2.3%) | 1 (0.8%) | 1.998 | 0.154 |
| Osteoporosis, n (%) | 9 (3.5%) | 0 (0%) | 9 (6.9%) | 5.040 | 0.024 |
| Management | |||||
| Steroids, n (%) | 100 (38.9%) | 42 (33.3%) | 58 (44.2%) | 3.234 | 0.072 |
| Anti-TNF, n (%) | 121 (47%) | 35 (27.7%) | 86 (65.6%) | 36.971 | <0.005 |
| Related surgeries, n (%) | 46 (17.8) | 3 (2.3%) | 43 (32.8%) | 40.506 | <0.005 |
| Abscess in Crohn’s Disease in Relation to the Location | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| L1 | L2 | L3 | L4 | |||||||||
| N | % | N | % | N | % | N | % | N | ||||
| Abscess | No | 33 | 27.3% | 18 | 14.9% | 68 | 56.2% | 2 | 1.7% | 121 | 0.516 | |
| Yes | 1 | 10.0% | 1 | 10.0% | 8 | 80.0% | 0 | 0.0% | 10 | |||
| Total | 34 | 26.0% | 19 | 14.5% | 76 | 58.0% | 2 | 1.5% | 131 | |||
| Fistula in Crohn’s Disease in Relation to the Location | Total | p | ||||||||||
| L1 | L2 | L3 | L4 | |||||||||
| N | % | N | % | N | % | N | % | N | ||||
| Fistula | No | 22 | 24.2% | 14 | 15.4% | 53 | 58.2% | 2 | 2.2% | 91 | 0.705 | |
| Yes | 12 | 30.0% | 5 | 12.5% | 23 | 57.5% | 0 | 0.0% | 40 | |||
| Total | 34 | 26.0% | 19 | 14.5% | 76 | 58.0% | 2 | 1.5% | 131 | |||
| Fissure in Crohn’s Disease in Relation to the Location | Total | p | ||||||||||
| L1 | L2 | L3 | L4 | |||||||||
| N | % | N | % | N | % | N | % | N | ||||
| Fissure | No | 32 | 26.2% | 16 | 13.1% | 72 | 59.0% | 2 | 1.6% | 122 | 0.412 | |
| Yes | 2 | 22.2% | 3 | 33.3% | 4 | 44.4% | 0 | 0.0% | 9 | |||
| Total | 34 | 26.0% | 19 | 14.5% | 76 | 58.0% | 2 | 1.5% | 131 | |||
| Fissure in Crohn’s Disease in Relation to Its Behavior | Total | p | |||||||
|---|---|---|---|---|---|---|---|---|---|
| B1 | B2 | B3 | |||||||
| N | % | N | % | N | % | N | |||
| Fissure | No | 68 | 56.2% | 28 | 23.1% | 25 | 20.7% | 121 | 0.117 |
| Yes | 2 | 22.2% | 3 | 33.3% | 4 | 44.4% | 9 | ||
| Total | 70 | 53.8% | 31 | 23.8% | 29 | 22.3% | 130 | ||
| Abscess in Crohn’s Disease in Relation to Its Behavior | Total | p | |||||||
| B1 | B2 | B3 | |||||||
| N | % | N | % | N | % | N | |||
| Abscess | No | 67 | 55.8% | 30 | 25% | 23 | 19.2% | 120 | 0.012 |
| Yes | 3 | 30% | 1 | 10% | 6 | 60% | 10 | ||
| Total | 70 | 53.8% | 31 | 23.8% | 29 | 22.3% | 130 | ||
| Fistula in Crohn’s Disease in Relation to Its Behavior | Total | p | |||||||
| B1 | B2 | B3 | |||||||
| N | % | N | % | N | % | N | |||
| Fistula | No | 55 | 61.1% | 22 | 24.4% | 13 | 14.4% | 90 | 0.004 |
| Yes | 15 | 37.5% | 9 | 22.5% | 16 | 40.0% | 40 | ||
| Total | 70 | 53.8% | 31 | 23.8% | 29 | 22.3% | 130 | ||
| Previous Surgery | Total | p | |||||
|---|---|---|---|---|---|---|---|
| No | Yes | ||||||
| N | % | N | % | N | |||
| Crohn’s Disease Behavior | B1 | 55 | 78.6% | 15 | 21.4% | 70 | 0.007 |
| B2 | 15 | 48.4% | 16 | 51.6% | 31 | ||
| B3 | 17 | 58.6% | 12 | 41.4% | 29 | ||
| Total | 87 | 66.9% | 43 | 33.1% | 130 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Fawzan, A.A.; Al-Radhi, S.A.; Al-Omar, A.S.; Al-Mutiri, N.H.; Al-Ammari, A.M.; El-Gohary, M.; Shamsan, A.N.; Al Shehri, H.M.; ALGhasab, N.S. A Study of the Epidemiology, Clinical, and Phenotypic Characteristics of Inflammatory Bowel Disease in the Northen-Central Region of Saudi Arabia. Diagnostics 2023, 13, 2135. https://doi.org/10.3390/diagnostics13132135
Al-Fawzan AA, Al-Radhi SA, Al-Omar AS, Al-Mutiri NH, Al-Ammari AM, El-Gohary M, Shamsan AN, Al Shehri HM, ALGhasab NS. A Study of the Epidemiology, Clinical, and Phenotypic Characteristics of Inflammatory Bowel Disease in the Northen-Central Region of Saudi Arabia. Diagnostics. 2023; 13(13):2135. https://doi.org/10.3390/diagnostics13132135
Chicago/Turabian StyleAl-Fawzan, Ahmed A., Sulaiman A. Al-Radhi, Ahmed S. Al-Omar, Nawaf H. Al-Mutiri, Ammar M. Al-Ammari, Mohammad El-Gohary, Amal N. Shamsan, Hamdan M. Al Shehri, and Naif S. ALGhasab. 2023. "A Study of the Epidemiology, Clinical, and Phenotypic Characteristics of Inflammatory Bowel Disease in the Northen-Central Region of Saudi Arabia" Diagnostics 13, no. 13: 2135. https://doi.org/10.3390/diagnostics13132135