
Effectiveness of Exercise in Patients with Overweight or Obesity Suffering from Knee Osteoarthritis: A Systematic Review and Meta-Analysis

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Criteria for Considering Studies for Inclusion in the Review
2.2. Protocol for Electronic Searching
2.3. Study Selection and Data Collection
2.4. Risk of Bias in Individual Studies
2.5. Statistical Analysis
3. Results
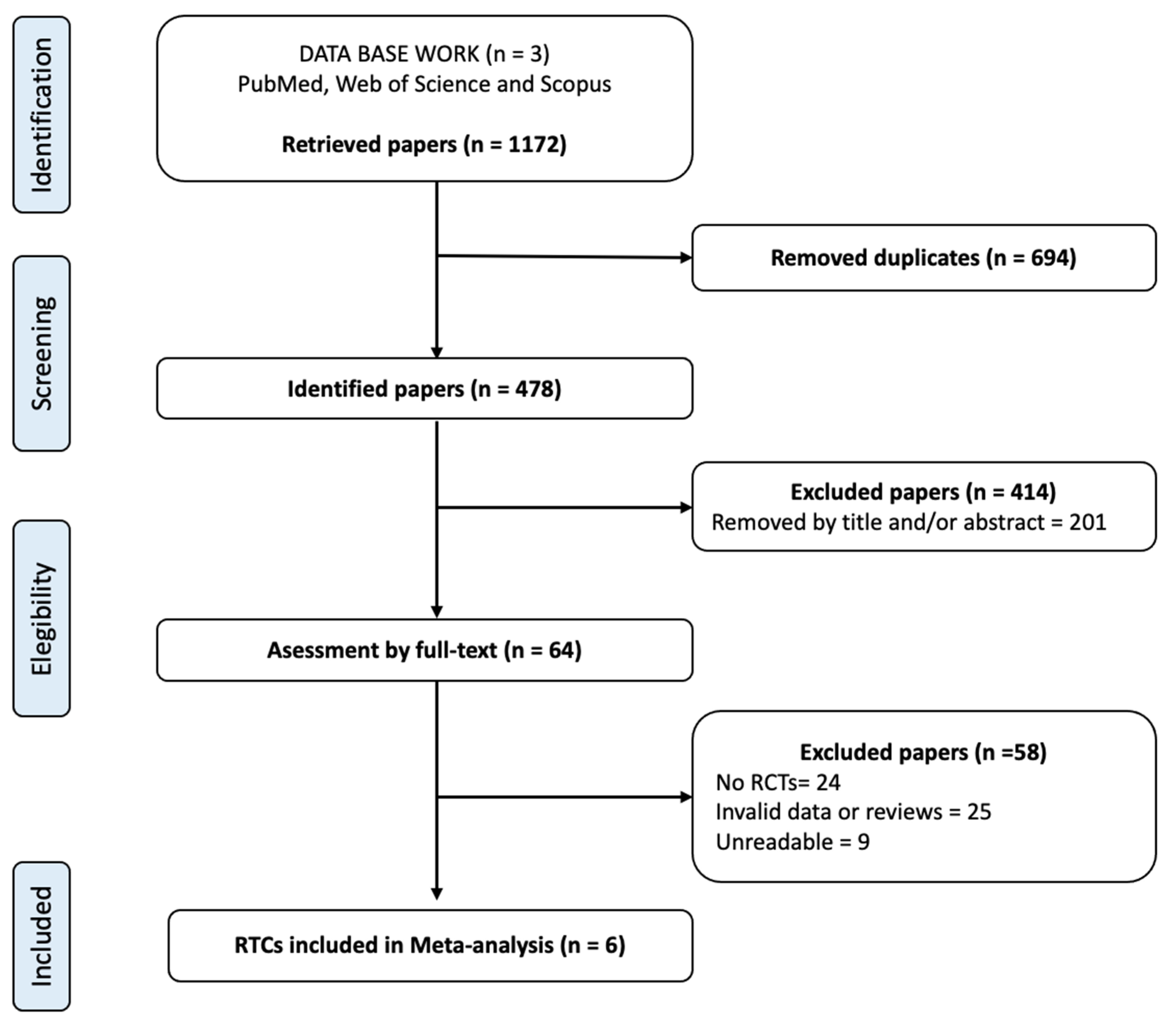
3.1. Studies Selected
3.2. Description of Selected Studies
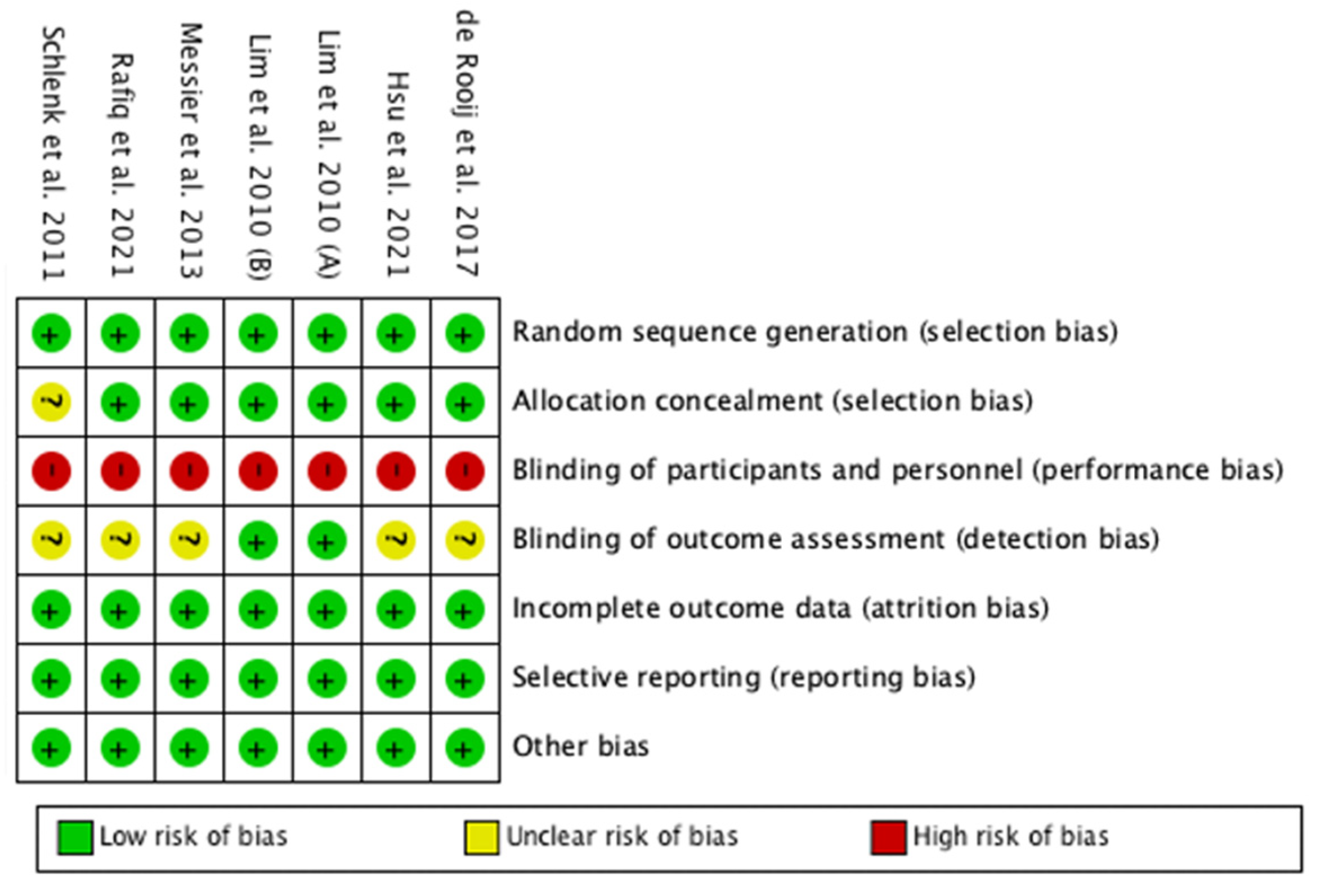
3.3. Risk of Bias in Included Studies
3.4. Effects of the Interventions
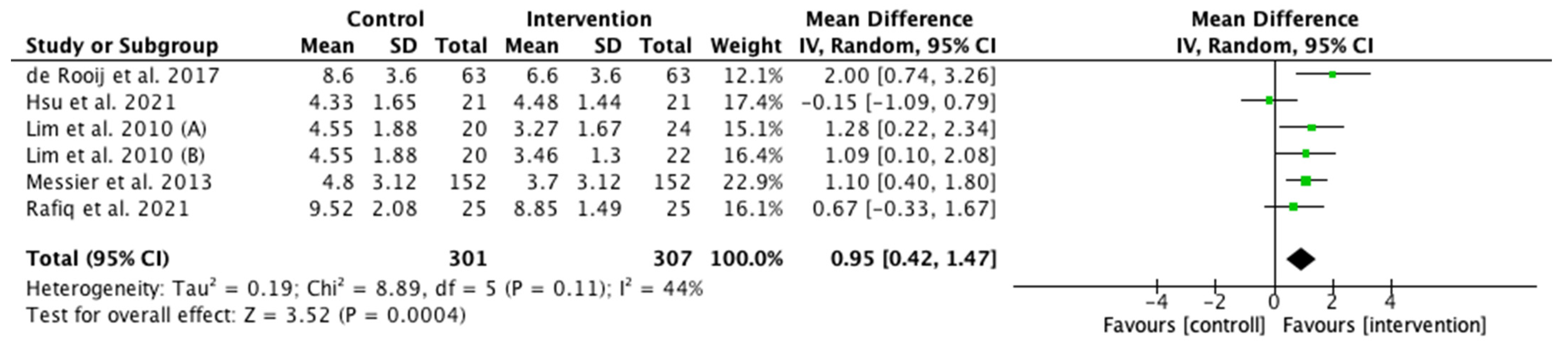
3.4.1. Pain
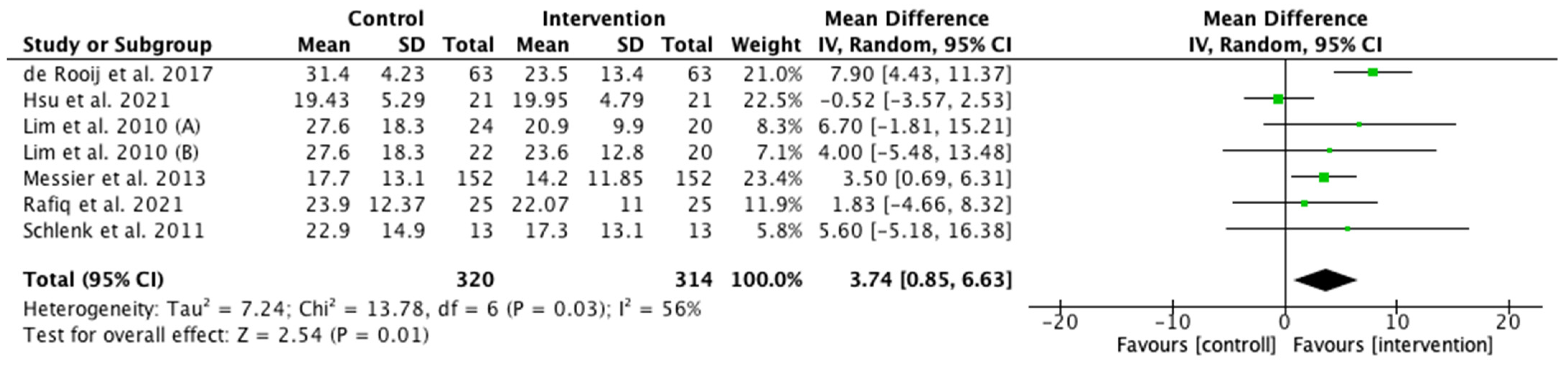
3.4.2. Physical function
3.4.3. Six-Minute Walk Test
3.5. Sensitivity Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Dantas, L.O.; de Fátima Salvini, T.; McAlindon, T.E. Knee osteoarthritis: Key treatments and implications for physical therapy. Braz. J. Phys. Ther. 2020, 25, 135–146. [Google Scholar] [CrossRef]
- Alrushud, A.S.; Rushton, A.B.; Kanavaki, A.M.; Greig, C.A. Effect of physical activity and dietary restriction interventions on weight loss and the musculoskeletal function of overweight and obese older adults with knee osteoarthritis: A systematic review and mixed method data synthesis. BMJ Open 2017, 7, e014537. [Google Scholar] [CrossRef]
- Hall, M.; Castelein, B.; Wittoek, R.; Calders, P.; van Ginckel, A. Diet-induced weight loss alone or combined with exercise in overweight or obese people with knee osteoarthritis: A systematic review and meta-analysis. Semin. Arthritis Rheum. 2019, 48, 765–777. [Google Scholar] [CrossRef]
- Loza, E.; Lopez-Gomez, J.M.; Abasolo, L.; Maese, J.; Carmona, L.; Batlle-Gualda, E.; Artrocad Study Group. Economic burden of knee and hip osteoarthritis in Spain. Arthritis Care Res. 2009, 61, 158–165. [Google Scholar] [CrossRef]
- Pages-Castella, A.; Alhambra, D.P. Artrosis, osteoporosis y fracturas: Controversias y evidencias. Med. Clin. 2013, 141, 217–220. [Google Scholar] [CrossRef]
- Pandya, N.K.; Draganich, L.F.; Mauer, A.; Piotrowski, G.A.; Pottenger, L. Osteoarthritis of the knees increases the propensity to trip on an obstacle. Clin. Orthop. Relat. Res. 2005, 431, 150–156. [Google Scholar] [CrossRef]
- Prieto-Alhambra, D.; Nogues, X.; Javaid, M.K.; Wyman, A.; Arden, N.K.; Azagra, R.; Cooper, C.; Adachi, J.D.; Boonen, S.; Chapurlat, R.D.; et al. An increased rate of falling leads to a rise in fracture risk in postmenopausal women with self-reported osteoarthritis: A prospective multinational cohort study (GLOW). Ann. Rheum. Dis. 2013, 72, 911–917. [Google Scholar] [CrossRef]
- Cartas, U.S.; Bejarano, S.J.C. Comorbidities and quality of life in Osteoarthritis. Rev. Cuba Reumatol. 2018, 20, 1–14. [Google Scholar]
- Batsis, J.A.; Zbehlik, A.J.; Barre, L.K.; Bynum, J.P.; Pidgeon, D.; Bartels, S.J. Impact of obesity on disability, function, and physical activity: Data from the Osteoarthritis Initiative. Scand. J. Rheumatol. 2015, 44, 495–502. [Google Scholar] [CrossRef]
- Ackerman, I.N.; Osborne, R.H. Obesity and increased burden of hip and knee joint disease in Australia: Results from a national survey. BMC Musculoskelet. Disord. 2012, 13, 254. [Google Scholar] [CrossRef]
- Ambrose, N.L.; Keogan, F.; O’Callaghan, J.P.; O’Connell, P.G. Obesity and disability in the symptomatic Irish knee osteoarthritis population. Ir. J. Med. Sci. 2010, 179, 265–268. [Google Scholar] [CrossRef]
- Vlietstra, L.; Stebbings, S.; Meredith-Jones, K.; Abbott, J.H.; Treharne, G.J.; Waters, D.L. Sarcopenia in osteoarthritis and rheumatoid arthritis: The association with self-reported fatigue, physical function and obesity. PLoS ONE 2019, 14, e0217462. [Google Scholar] [CrossRef]
- Cho, B.Y.; Seo, D.C.; Lin, H.C.; Lohrmann, D.K.; Chomistek, A.K. BMI and Central Obesity with Falls among Community-Dwelling Older Adults. Am. J. Prev. Med. 2018, 54, e59–e66. [Google Scholar] [CrossRef]
- Fransen, M.; McConnell, S.; Harmer, A.R.; van der Esch, M.; Simic, M.; Bennell, K.L. Exercise for osteoarthritis of the knee: A Cochrane systematic review. Br. J. Sports Med. 2015, 49, 1554–1557. [Google Scholar] [CrossRef]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 9, CD007146. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Hendrix, I.C. RefWorks. J. Med. Libr. Assoc. 2004, 92, 111. [Google Scholar]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Collins, N.J.; Misra, D.; Felson, D.T.; Crossley, K.M.; Roos, E.M. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis Care Res. 2011, 63, S208–S228. [Google Scholar]
- Rikli, R.E.; Jones, C.J. Development and validation of a functional fitness test for community-residing older adults. J. Aging Phys. Activ. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Takkouche, B.; Cadarso-Suárez, C.; Spiegelman, D. Evaluation of old and new tests of heterogeneity in epidemiologic meta-analysis. Am. J. Epidemiol. 1999, 150, 206–215. [Google Scholar] [CrossRef]
- Higgins, J.P.T.T.J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3; Updated February 2022; Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 5 May 2022).
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; SAGE Publishing: Los Angeles, CA, USA, 2015. [Google Scholar]
- Cochrane, T. Review Manager (RevMan) 5.3; The Nordic Cochrane Centre: Copenhagen, Denmark, 2008. [Google Scholar]
- Messier, S.P.; Mihalko, S.L.; Legault, C.; Miller, G.D.; Nicklas, B.J.; DeVita, P.; Beavers, D.P.; Hunter, D.J.; Lyles, M.F.; Eckstein, F.; et al. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: The IDEA randomized clinical trial. JAMA 2013, 310, 1263–1273. [Google Scholar] [CrossRef]
- Schlenk, E.A.; Lias, J.L.; Sereika, S.M.; Dunbar-Jacob, J.; Kwoh, C.K. Improving physical activity and function in overweight and obese older adults with osteoarthritis of the knee: A feasibility study. Rehabil. Nurs. 2011, 36, 32–42. [Google Scholar] [CrossRef] [PubMed]
- De Rooij, M.; van der Leeden, M.; Cheung, J.; van der Esch, M.; Häkkinen, A.; Haverkamp, D.; Roorda, L.D.; Twisk, J.; Vollebregt, J.; Lems, W.F.; et al. Efficacy of Tailored Exercise Therapy on Physical Functioning in Patients with Knee Osteoarthritis and Comorbidity: A Randomized Controlled Trial. Arthritis Rheum. 2017, 69, 807–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, Y.I.; Chen, Y.C.; Lee, C.L.; Chang, N.J. Effects of Diet Control and Telemedicine-Based Resistance Exercise Intervention on Patients with Obesity and Knee Osteoarthritis: A Randomized Control Trial. Int. J. Environ. Res. Public Health 2021, 18, 7744. [Google Scholar] [CrossRef]
- Lim, J.Y.; Tchai, E.; Jang, S.N. Effectiveness of aquatic exercise for obese patients with knee osteoarthritis: A randomized controlled trial. Pm&r 2010, 2, 723–731. [Google Scholar]
- Rafiq, M.T.; Hamid, M.S.A.; Hafiz, E. Short-Term Effects of Strengthening Exercises of the Lower Limb Rehabilitation Protocol on Pain, Stiffness, Physical Function, and Body Mass Index among Knee Osteoarthritis Participants Who Were Overweight or Obese: A Clinical Trial. Sci. World J. 2021, 22, 6672274. [Google Scholar] [CrossRef]
- Araujo, C.G.; de Souza, C.G.; Laukkanen, J.A.; Singh, M.F.; Kunutsor, S.K.; Myers, J.; Franca, J.P.; Castro, C.L. Successful 10-s one-legged stance performance predicts survival in middle-aged and older individuals. Br. J. Sports Med. 2022, 105360. [Google Scholar] [CrossRef]
- Oliveira, A.M.; Peccin, M.S.; Silva, K.N.; Teixeira, L.E.; Trevisani, V.F. Impact of exercise on the functional capacity and pain of patients with knee osteoarthritis: A radomized clinical trial. Rev. Bras. Reumatol. 2012, 6, 876–882. [Google Scholar] [CrossRef]
- Imoto, A.; Peccin, M.; Trevisani, V. Quadriceps strengthening exercises are effective in improving pain, function and quality of life in patients with osteoarthritis of the knee. Acta Ortop. Bras. 2012, 20, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Topp, R.; Woolley, S.; Hornyak, J., 3rd; Khuder, S.; Kahaleh, B. The effect of dynamic versus isometric resistance training on pain and functioning among adults with osteoarthritis of the knee. Arch. Phys. Med. Rehabil. 2002, 83, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Lai, Z.; Wang, L. Effects of Taichi exercise on knee and ankle proprioception among individuals with knee osteoarthritis. Res. Sports Med. 2019, 28, 268–278. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Suzuki, T.; Saito, K.; Kim, M.; Kojima, N.; Ishizaki, T.; Yamashiro, Y.; Hosoi, E.; Yoshida, H. Effectiveness of exercise with or without thermal therapy for community-dwelling elderly Japanese women with non-specific knee pain: A randomized controlled trial. Arch. Gerontol. Geriatr. 2013, 3, 352–359. [Google Scholar] [CrossRef]
- Chen, H.; Wang, Y.; Liu, C.; Lu, H.; Liu, N.; Yu, F.; Wan, Q.; Chen, J.; Shang, S. Benefits of a transtheoretical model-based program on exercise adherence in older adults with knee osteoarthritis: A cluster randomized controlled trial. J. Adv. Nurs. 2020, 76, 1765–1779. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Lee, Y.; Shin, S. The Effect of Body Composition on Gait Variability Varies with Age: Interaction by Hierarchical Moderated Regression Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1171. [Google Scholar] [CrossRef]
- Jin, W.S.; Choi, E.J.; Lee, S.Y.; Bae, E.J.; Lee, T.H.; Park, J. Relationships among Obesity, Sarcopenia, and Osteoarthritis in the Elderly. J. Obes. Metab. Syndr. 2017, 26, 36–44. [Google Scholar] [CrossRef]
- Alshami, A.M.; Alhassany, H.A. Girth, strength, and flexibility of the calf muscle in patients with knee osteoarthritis: A case-control study. J. Taibah Univ. Med. Sci. 2020, 15, 197–202. [Google Scholar] [CrossRef]
- Loureiro, A.; Constantinou, M.; Diamond, L.E.; Beck, B.; Barrett, R. Individuals with mild-to-moderate hip osteoarthritis have lower limb muscle strength and volume deficits. BMC Musculoskelet. Disord. 2018, 19, 303. [Google Scholar] [CrossRef]
- Jeon, H.; Lee, S.U.; Lim, J.Y.; Chung, S.G.; Lee, S.J.; Lee, S.Y. Low skeletal muscle mass and radiographic osteoarthritis in knee, hip, and lumbar spine: A cross-sectional study. Aging Clin. Exp. Res. 2019, 31, 1557–1562. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Pan, X.; Deng, L.; Fu, W. Relationship between Knee Muscle Strength and Fat/Muscle Mass in Elderly Women with Knee Osteoarthritis based on Dual-Energy X-ray Absorptiometry. Int. J. Environ. Res. Public Health 2020, 17, 573. [Google Scholar] [CrossRef] [PubMed]
- Park, H.M.; Kim, H.J.; Lee, B.; Kwon, M.; Jung, S.M.; Lee, S.W.; Park, Y.B.; Song, J.J. Decreased muscle mass is independently associated with knee pain in female patients with radiographically mild osteoarthritis: A nationwide cross-sectional study (KNHANES 2010–2011). Clin. Rheumatol. 2018, 37, 1333–1340. [Google Scholar] [CrossRef]
- Cheon, Y.H.; Kim, H.O.; Suh, Y.S.; Kim, M.G.; Yoo, W.H.; Kim, R.B.; Yang, H.S.; Lee, S.I.; Park, K.S. Relationship between decreased lower extremity muscle mass and knee pain severity in both the general population and patients with knee osteoarthritis: Findings from the KNHANES V 1-2. PLoS ONE 2017, 12, e0173036. [Google Scholar] [CrossRef] [PubMed]
- Pickering, M.E.; Chapurlat, R. Where Two Common Conditions of Aging Meet: Osteoarthritis and Sarcopenia. Calcif. Tissue Int. 2020, 107, 203–211. [Google Scholar] [CrossRef]
- Shorter, E.; Sannicandro, A.J.; Poulet, B.; Goljanek-Whysall, K. Skeletal Muscle Wasting and Its Relationship with Osteoarthritis: A Mini-Review of Mechanisms and Current Interventions. Curr. Rheumatol. Rep. 2019, 21, 40. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Duchowny, K.A.; Peters, K.E.; Cummings, S.R.; Orwoll, E.S.; Hoffman, A.R.; Ensrud, K.E.; Cauley, J.A.; Evans, W.J.; Cawthon, P.M. Association of change in muscle mass assessed by D3-creatine dilution with changes in grip strength and walking speed. J. Cachexia Sarcopenia Muscle 2020, 11, 55–61. [Google Scholar] [CrossRef]
- Osawa, Y.; Chiles Shaffer, N.; Shardell, M.D.; Studenski, S.A.; Ferrucci, L. Changes in knee extension peak torque and body composition and their relationship with change in gait speed. J. Cachexia Sarcopenia Muscle 2019, 10, 1000–1008. [Google Scholar] [CrossRef]
- Liao, C.D.; Chen, H.C.; Huang, S.W.; Liou, T.H. The Role of Muscle Mass Gain Following Protein Supplementation Plus Exercise Therapy in Older Adults with Sarcopenia and Frailty Risks: A Systematic Review and Meta-Regression Analysis of Randomized Trials. Nutrients 2019, 11, 1713. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef] [PubMed]
- Yogi, R.R.; Sammy, I.; Paul, J.F.; Nunes, P.; Robertson, P.; Ramcharitar Maharaj, V. Falls in Older People: Comparing Older and Younger Fallers in a Developing Country. Eur. J. Trauma Emerg. Surg. 2018, 44, 567–571. [Google Scholar] [CrossRef]
- Chu, S.-F.; Liou, T.-H.; Chen, H.-C.; Huang, S.-W.; Liao, C.-D. Relative Efficacy of Weight Management, Exercise, and Combined Treatment for Muscle Mass and Physical Sarcopenia Indices in Adults with Overweight or Obesity and Osteoarthritis: A Network Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 1992. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Kang, S.H.; Choi, H.G. Analysis of the Associations between Arthritis and Fall Histories in Korean Adults. Int. J. Environ. Res. Public Health 2021, 18, 3758. [Google Scholar] [CrossRef] [PubMed]
- McAlindon, T. Osteoarthritis Research Society International (OARSI) Classification and Guidelines. HSS J. 2012, 8, 66–67. [Google Scholar] [CrossRef]
- Siedentopp, U. Tratamiento dietético integrador para la artrosis y la osteoporosis. Rev. Int. Acupunt. 2011, 5, 13–17. [Google Scholar] [CrossRef]
- Henriksen, M.; Christensen, R.; Danneskiold-Samsøe, B.; Bliddal, H. Changes in lower extremity muscle mass and muscle strength after weight loss in obese patients with knee osteoarthritis: A prospective cohort study. Arthritis Rheum. 2012, 64, 438–442. [Google Scholar] [CrossRef]
- Pazzianotto-Forti, E.M.; Moreno, M.A.; Plater, E.; Baruki, S.B.S.; Rasera-Junior, I.; Reid, W.D. Impact of Physical Training Programs on Physical Fitness in People with Class II and III Obesity: A Systematic Review and Meta-Analysis. Phys. Ther. 2020, 100, 963–978. [Google Scholar] [CrossRef]
- Van Gool, C.H.; Penninx, B.W.J.H.; Kempen, G.I.J.M.; Rejeski, W.J.; Miller, G.D.; van Eijk, J.T.M.; Pahor, M.; Messier, S.P. Effects of exercise adherence on physical function among overweight older adults with knee osteoarthritis. Arthritis Rheum. 2005, 53, 24–32. [Google Scholar] [CrossRef]
- American Academy of Orthopaedic Surgeons. Management of Osteoarthritis of the Knee (Non-Arthroplasty). Evidence-Based Clinical Practice Guideline. Available online: https://www.aaos.org/oak3cpg (accessed on 5 May 2022).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Group | Sample (n) | BMI | Treatment Length | Treatment Exercise Intervention | Main Results |
|---|---|---|---|---|---|---|---|
| De Rooij et al., 2017 [28] | Netherlands | Non-Intervention | 42 | 35 ± 7.6 | 12 months | Individualized, comorbidity-adapted exercise program consisting of aerobic and strength training and training of daily activities. The control group received their current medical care for KO and were placed on a waiting list for exercise therapy. | At 3 months follow-up, the mean improvements in the intervention group were 33% on the WOMAC scale and 15% on the 6MWT. Tailored exercise therapy is efficacious in improving physical functioning in patients with KO and severe comorbidities. |
| Intervention | 60 | 36 ± 6.8 | |||||
| Hsu et al., 2021 [29] | China | Non-Intervention | 21 | 29.45 ± 2.59 | 12 months | An elastic band resistance exercise intervention was implemented. Each participant performed 10 repetitions/set of five sets/day of the aforementioned exercise movements 3 days a week for 12 weeks. Exercise intensity was increased by applying more force to the band to provide greater resistance or by switching to a thicker resistance band that created more resistance and thus increased exercise difficulty. A repetition maximum of 10 and rated perceived exertion of 13 (range of 6–20) were applied as the standards for the exercise program. | Individual diet control intervention combined with telemedicine-based resistance exercise intervention significantly improved the body composition, blood biochemistry, and lower-limb functional performance of the investigated population with comorbid conditions. |
| Intervention | 21 | 29.7 ± 2.64 | |||||
| Lim et al., 2010 (A) [30] | Korea | Non-Intervention | 20 | 27.86 ± 1.99 | 2 months | Each training session consisted of main activities in an aquatic gym for 30 min. The exercise program always started with 5 min of warm-up and ended with 5 min of cooldown. The exercise program was designed with 40 min duration per session, 3 times per week, for 8 weeks. Exercise intensity was maintained at the level of more than 65% of maximal heart rate by checking subject heart rates intermittently during exercise. | After the exercise intervention, BMI showed a small reduction in water exercise group. There was an enhancement in functional performance. Water exercise reduced the degree of activity interference by pain. Thus, water exercise may be an effective tool for patients with obesity who have difficulty in conventional exercises because of combined KO. |
| Intervention | 24 | 27.82 ± 1.56 | |||||
| Lim et al., 2010 (B) [30] | Korea | Non-Intervention | 20 | 27.86 ± 1.99 | 2 months | Participants assigned to the 8-week land-based exercise program underwent a generalized conditioning program also with knee specific exercises. Exercise duration was 40 min in each session, including 5 min of warm-up and 5 min of cooldown. The intensity of exercise began from 40% of the 1-repetition maximum for the beginner, but in advanced classes, 60% of 1-repetition maximum was applied, which is the usual intensity for geriatric patients. The exercises consisted of joint mobilization and strengthening exercises. Range-of-motion and stretching exercises of the hamstring, rectus femoris, tensor fascia latae, and calf muscles were included. Bicycling was also included for aerobic conditioning and fitness. A quadriceps isometric strengthening exercise was performed, along with other strengthening exercises, such as leg presses and leg extensions. | BMI showed a small reduction in exercise group. There was an enhancement in functional performance. |
| Intervention | 22 | 27.49 ± 1.66 | |||||
| Messier et al., 2013 [26] | USA | Non-Intervention | 52 | 33.7 ± 3.8 | 18 months | The exercise intervention was conducted for 1 h on 3 days/week. During the first 6 months, participation was center-based. After 6-month follow-up testing and a 2-week transition phase, participants could remain in the facility program, opt for a home-based program, or combine the two. The program consisted of aerobic walking (15 min), strength training (20 min), a second aerobic phase (15 min), and cool-down (10 min) | Compared with exercise participants, knee compressive forces were lower in diet participants, and IL-6 were lower in diet and diet + exercise participants. Pairwise between-group comparisons of WOMAC pain and function at 18 months revealed that the diet and exercise group had less pain relative to the exercise and diet groups. Pairwise between-group comparison showed that WOMAC function score was significantly better in the diet and exercise group relative to the exercise group. |
| Intervention | 52 | 33.6 ± 3.7 | |||||
| The 6MWT distance was 23.3 m farther in the diet and exercise group relative to the exercise group. | |||||||
| Rafiq et al., 2021 [31] | Malaysia | Non-Intervention | 25 | 32.01 ± 3.89 | 1 month | Training sessions included strengthening exercises for the lower limbs in non-weight-bearing, sitting, or lying positions. Each training session started with 10 min of warm-up, 45–60 min of lower-limb resistance training, and 10 min of cooldown at the end of the training protocol. A cooldown period is essential after a training session and should last approximately 5–10 min. When static stretching is used as a part of warm-up immediately prior to exercise, it causes harm to muscle strength. | Short-term effects of the lower-limb rehabilitation protocol appear to reduce knee pain and stiffness only, but not physical function and BMI. |
| Intervention | 25 | 32.18 ± 4.49 | |||||
| Schlenk et al., 2011 [27] | USA | Non-Intervention | 13 | 33.3 ± 6 | 6 months | A fitness walking program was initiated in the fifth session (previous sessions consisted of a standardized educational program on sedentary lifestyles and obesity as risk factors for cardiovascular disease and KO) with the physical therapist to gradually progress subjects to fitness walking within their limitations, taking into account their symptoms. Subjects were to walk toward a goal of 150 min per week, but were permitted to distribute this time among multiple sessions as tolerated or preferred. The fitness walking program promoted performance of physical activity by graduated fitness walking goals, demonstration, and practice consistent with the self-efficacy strategy of mastery. | Results showed significant increases in self-reported performance of lower extremity exercise and participation in fitness walking, 6MWT distance, and Short Physical Performance Battery scores from baseline to 6-month follow-up with a trend of improvement in self-efficacy. Results suggest that the intervention was feasible, acceptable, and improved physical activity and function. |
| Intervention | 13 | (Reported for both groups) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurado-Castro, J.M.; Muñoz-López, M.; Ledesma, A.S.-T.; Ranchal-Sanchez, A. Effectiveness of Exercise in Patients with Overweight or Obesity Suffering from Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 10510. https://doi.org/10.3390/ijerph191710510
Jurado-Castro JM, Muñoz-López M, Ledesma AS-T, Ranchal-Sanchez A. Effectiveness of Exercise in Patients with Overweight or Obesity Suffering from Knee Osteoarthritis: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(17):10510. https://doi.org/10.3390/ijerph191710510
Chicago/Turabian StyleJurado-Castro, Jose Manuel, Mariano Muñoz-López, Agustín Sánchez-Toledo Ledesma, and Antonio Ranchal-Sanchez. 2022. "Effectiveness of Exercise in Patients with Overweight or Obesity Suffering from Knee Osteoarthritis: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 17: 10510. https://doi.org/10.3390/ijerph191710510