Surgical Care
Most cavernous angiomas require no intervention. If surgical extirpation is indicated, the approach to the orbit is dictated by tumor location within the orbit. [5]
Most cavernous angiomas are found between the optic nerve and extraocular muscles within the intraconal space. A lateral orbitotomy, or a variant thereof, is a typical approach. Tumors within the medial aspect of the orbit are approached best through an upper eyelid or a transcaruncular-based medial orbitotomy. Additionally, an anterior orbitotomy via a lower eyelid transconjunctival approach can be used. This approach was used for removal of intraconal hemangiomas extending to the orbital apex. [6]
 MRI demonstrates enhancing mass in apex of left orbit. White arrow points to the superior portion of the optic nerve, showing its deviation. Mass was pressing on superotemporal optic nerve and displacing it inferomedially at apex. Patient had 6 months of progressive decreased vision and visual field loss. Courtesy of M. Duffy, MD, PhD.
MRI demonstrates enhancing mass in apex of left orbit. White arrow points to the superior portion of the optic nerve, showing its deviation. Mass was pressing on superotemporal optic nerve and displacing it inferomedially at apex. Patient had 6 months of progressive decreased vision and visual field loss. Courtesy of M. Duffy, MD, PhD.
 In A, final preoperative visual field of same patient as in Media file 2, demonstrating significant inferior altitudinal field loss; in B, postoperative visual field at approximately 3 weeks after orbital apex decompression and removal of mass; and in C, postoperative visual field at approximately 6 months.
In A, final preoperative visual field of same patient as in Media file 2, demonstrating significant inferior altitudinal field loss; in B, postoperative visual field at approximately 3 weeks after orbital apex decompression and removal of mass; and in C, postoperative visual field at approximately 6 months.
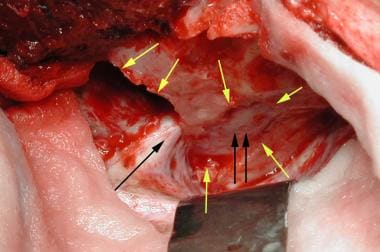 Intraoperative photo of same patient as in Media file 2. Neurosurgical service performed craniotomy and decompression of the superior orbital fissure and optic canal (yellow arrows) at request of ophthalmology service. Orbital surgery service then opened the periorbita over a bulge (double black arrows) between optic nerve and cranial nerves (single black arrow) and bluntly dissected out mass. Pathology confirmed mass as a cavernous hemangioma. Cranial nerves V and IV were adhered, and careful blunt separation was performed. Postoperatively, a small left hypertropia resolved over 6 weeks. Courtesy of M. Duffy, MD, PhD.
Intraoperative photo of same patient as in Media file 2. Neurosurgical service performed craniotomy and decompression of the superior orbital fissure and optic canal (yellow arrows) at request of ophthalmology service. Orbital surgery service then opened the periorbita over a bulge (double black arrows) between optic nerve and cranial nerves (single black arrow) and bluntly dissected out mass. Pathology confirmed mass as a cavernous hemangioma. Cranial nerves V and IV were adhered, and careful blunt separation was performed. Postoperatively, a small left hypertropia resolved over 6 weeks. Courtesy of M. Duffy, MD, PhD.
After adequate exposure, a well-circumscribed, purple, encapsulated lesion is seen with distinct vessels on its surface. Gentle blunt dissection allows for en-bloc removal after all vessels have been identified and cauterized with bipolar cautery.
 Extirpation of an orbital cavernous hemangioma. Note en bloc removal and preservation of capsule. Courtesy of Robert Alan Goldberg, MD.
Extirpation of an orbital cavernous hemangioma. Note en bloc removal and preservation of capsule. Courtesy of Robert Alan Goldberg, MD.
The cryoprobe allows for removal of well-circumscribed lesions, reducing the incidence of capsular rupture and bleeding, making it an ideal tool for hemangioma extirpation. A disadvantage of the cryoprobe is that adjacent orbital structures also may be frozen, as is the case with deep orbital tumors.
Use of the carbon dioxide laser or Nd:YAG laser is another modality for the surgeon faced with the task of tumor removal.
Gamma knife surgery has been used with success. Liu et al found gamma knife surgery to be an effective treatment in 23 patients with orbital cavernous hemangiomas. [7]
Consultations
If the cavernous hemangioma has an intracranial component or extends to facial structures outside the orbit, neurosurgical or otolaryngologic consultation should be sought.
-
Extirpation of an orbital cavernous hemangioma. Note en bloc removal and preservation of capsule. Courtesy of Robert Alan Goldberg, MD.
-
MRI demonstrates enhancing mass in apex of left orbit. White arrow points to the superior portion of the optic nerve, showing its deviation. Mass was pressing on superotemporal optic nerve and displacing it inferomedially at apex. Patient had 6 months of progressive decreased vision and visual field loss. Courtesy of M. Duffy, MD, PhD.
-
In A, final preoperative visual field of same patient as in Media file 2, demonstrating significant inferior altitudinal field loss; in B, postoperative visual field at approximately 3 weeks after orbital apex decompression and removal of mass; and in C, postoperative visual field at approximately 6 months.
-
Intraoperative photo of same patient as in Media file 2. Neurosurgical service performed craniotomy and decompression of the superior orbital fissure and optic canal (yellow arrows) at request of ophthalmology service. Orbital surgery service then opened the periorbita over a bulge (double black arrows) between optic nerve and cranial nerves (single black arrow) and bluntly dissected out mass. Pathology confirmed mass as a cavernous hemangioma. Cranial nerves V and IV were adhered, and careful blunt separation was performed. Postoperatively, a small left hypertropia resolved over 6 weeks. Courtesy of M. Duffy, MD, PhD.


