[Guideline] Knopman DS, DeKosky ST, Cummings JL, Chui H, Corey-Bloom J, Relkin N, et al. Practice parameter: diagnosis of dementia (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001 May 8. 56(9):1143-53. [QxMD MEDLINE Link]. [Full Text].
Mosconi L, Berti V, Glodzik L, Pupi A, De Santi S, de Leon MJ. Pre-clinical detection of Alzheimer's disease using FDG-PET, with or without amyloid imaging. J Alzheimers Dis. 2010. 20 (3):843-54. [QxMD MEDLINE Link].
Winslow BT, Onysko MK, Stob CM, Hazlewood KA. Treatment of Alzheimer disease. Am Fam Physician. 2011 Jun 15. 83(12):1403-12. [QxMD MEDLINE Link].
Massoud F, Léger GC. Pharmacological treatment of Alzheimer disease. Can J Psychiatry. 2011 Oct. 56(10):579-88. [QxMD MEDLINE Link].
Madhusoodanan S, Shah P, Brenner R, Gupta S. Pharmacological treatment of the psychosis of Alzheimer's disease: what is the best approach?. CNS Drugs. 2007. 21(2):101-15. [QxMD MEDLINE Link].
Rolland Y, Abellan van Kan G, Vellas B. Healthy brain aging: role of exercise and physical activity. Clin Geriatr Med. 2010 Feb. 26(1):75-87. [QxMD MEDLINE Link].
Honea RA, Thomas GP, Harsha A, Anderson HS, Donnelly JE, Brooks WM, et al. Cardiorespiratory fitness and preserved medial temporal lobe volume in Alzheimer disease. Alzheimer Dis Assoc Disord. 2009 Jul-Sep. 23(3):188-97. [QxMD MEDLINE Link]. [Full Text].
Brookmeyer R, Abdalla N, Kawas CH, Corrada MM. Forecasting the prevalence of preclinical and clinical Alzheimer's disease in the United States. Alzheimers Dement. 2017 Nov 29. [QxMD MEDLINE Link].
Taylor CA, Greenlund SF, McGuire LC, Lu H, Croft JB. Deaths from Alzheimer's Disease - United States, 1999-2014. MMWR Morb Mortal Wkly Rep. 2017 May 26. 66 (20):521-526. [QxMD MEDLINE Link].
Alzheimer's Association. 2017 Alzheimer's disease facts and figures. Alzheimers Dement. 2017. 13:325-373.
Maurer K, Maurer U. Alzheimer: The Life of a Physician and Career of a Disease. New York: Columbia University Press; 2003.
Alzheimer A. Uber eine eigenartige Erkangkung der Hirnrinde. Allgemeine Zeitschrift fur Psychiatrie und Psychisch-Gerichtliche Medizin. 1907. 64: 146-148.
Braak H, Braak E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol. 1991. 82(4):239-59. [QxMD MEDLINE Link].
Serrano-Pozo A, Frosch MP, Masliah E, Hyman BT. Neuropathological alterations in Alzheimer disease. Cold Spring Harb Perspect Biol. 2011 Sep. 3(9):a006189. [QxMD MEDLINE Link].
Brayne C, Richardson K, Matthews FE, et al. Neuropathological correlates of dementia in over-80-year-old brain donors from the population-based Cambridge city over-75s cohort (CC75C) study. J Alzheimers Dis. 2009. 18(3):645-58. [QxMD MEDLINE Link].
Gordon BA, Blazey TM, Su Y, Hari-Raj A, Dincer A, et al. Spatial patterns of neuroimaging biomarker change in individuals from families with autosomal dominant Alzheimer's disease: a longitudinal study. Lancet Neurol. 2018 Mar. 17 (3):241-250. [QxMD MEDLINE Link].
Swerdlow RH, Khan SM. The Alzheimer's disease mitochondrial cascade hypothesis: an update. Exp Neurol. 2009 Aug. 218(2):308-15. [QxMD MEDLINE Link]. [Full Text].
Nelson PT, Dickson DW, Trojanowski JQ, et al. Limbic-predominant age-related TDP-43 encephalopathy (LATE): consensus working group report. Brain. 2019 Apr 30. [QxMD MEDLINE Link].
Braak H, Thal DR, Ghebremedhin E, Del Tredici K. Stages of the pathologic process in Alzheimer disease: age categories from 1 to 100 years. J Neuropathol Exp Neurol. 2011 Nov. 70(11):960-9. [QxMD MEDLINE Link].
Braak H, Braak E, Grundke-Iqbal I, Iqbal K. Occurrence of neuropil threads in the senile human brain and in Alzheimer's disease: a third location of paired helical filaments outside of neurofibrillary tangles and neuritic plaques. Neurosci Lett. 1986 Apr 24. 65(3):351-5. [QxMD MEDLINE Link].
Davinelli S, Intrieri M, Russo C, Di Costanzo A, Zella D, Bosco P, et al. The "Alzheimer's disease signature": potential perspectives for novel biomarkers. Immun Ageing. 2011 Sep 20. 8:7. [QxMD MEDLINE Link]. [Full Text].
Higgins GC, Beart PM, Shin YS, Chen MJ, Cheung NS, Nagley P. Oxidative stress: emerging mitochondrial and cellular themes and variations in neuronal injury. J Alzheimers Dis. 2010. 20 Suppl 2:S453-73. [QxMD MEDLINE Link].
Ding Q, Dimayuga E, Keller JN. Oxidative damage, protein synthesis, and protein degradation in Alzheimer's disease. Curr Alzheimer Res. 2007 Feb. 4(1):73-9. [QxMD MEDLINE Link].
Thambisetty M, Simmons A, Velayudhan L, Hye A, Campbell J, Zhang Y, et al. Association of plasma clusterin concentration with severity, pathology, and progression in Alzheimer disease. Arch Gen Psychiatry. 2010 Jul. 67(7):739-48. [QxMD MEDLINE Link].
Schrijvers EM, Koudstaal PJ, Hofman A, Breteler MM. Plasma clusterin and the risk of Alzheimer disease. JAMA. 2011 Apr 6. 305(13):1322-6. [QxMD MEDLINE Link].
Shumaker SA, Legault C, Rapp SR, Thal L, Wallace RB, Ockene JK, et al. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women's Health Initiative Memory Study: a randomized controlled trial. JAMA. 2003 May 28. 289(20):2651-62. [QxMD MEDLINE Link].
Xu W, Tan L, Wang HF, Jiang T, Tan MS, Tan L, et al. Meta-analysis of modifiable risk factors for Alzheimer's disease. J Neurol Neurosurg Psychiatry. 2015 Dec. 86 (12):1299-306. [QxMD MEDLINE Link].
Rocchi A, Orsucci D, Tognoni G, Ceravolo R, Siciliano G. The role of vascular factors in late-onset sporadic Alzheimer's disease. Genetic and molecular aspects. Curr Alzheimer Res. 2009 Jun. 6(3):224-37. [QxMD MEDLINE Link].
S Roriz-Filho J, Sá-Roriz TM, Rosset I, Camozzato AL, Santos AC, Chaves ML, et al. (Pre)diabetes, brain aging, and cognition. Biochim Biophys Acta. 2009 May. 1792(5):432-43. [QxMD MEDLINE Link].
Naderali EK, Ratcliffe SH, Dale MC. Obesity and Alzheimer's disease: a link between body weight and cognitive function in old age. Am J Alzheimers Dis Other Demen. 2009 Dec-2010 Jan. 24(6):445-9. [QxMD MEDLINE Link].
de la Monte SM. Insulin resistance and Alzheimer's disease. BMB Rep. 2009 Aug 31. 42(8):475-81. [QxMD MEDLINE Link].
Hughes S. Beta-Blockers Linked to Fewer Alzheimer's Lesions. Available at http://www.medscape.com/viewarticle/777239. Accessed: January 15, 2013.
Perl DP. Relationship of aluminum to Alzheimer's disease. Environ Health Perspect. 1985 Nov. 63:149-53. [QxMD MEDLINE Link]. [Full Text].
Perl DP, Moalem S. Aluminum and Alzheimer's disease, a personal perspective after 25 years. J Alzheimers Dis. 2006. 9(3 Suppl):291-300. [QxMD MEDLINE Link].
Anderson, P. Early-Life Depression Boosts Alzheimer's Risk. Medscape Medical News. Available at http://www.medscape.com/viewarticle/883327. July 24, 2017; Accessed: July 26, 2017.
Goldbourt U, Schnaider-Beeri M, Davidson M. Socioeconomic status in relationship to death of vascular disease and late-life dementia. J Neurol Sci. 2007 Jun 15. 257(1-2):177-81. [QxMD MEDLINE Link].
McDowell I, Xi G, Lindsay J, Tierney M. Mapping the connections between education and dementia. J Clin Exp Neuropsychol. 2007 Feb. 29(2):127-41. [QxMD MEDLINE Link].
Szekely CA, Zandi PP. Non-steroidal anti-inflammatory drugs and Alzheimer's disease: the epidemiological evidence. CNS Neurol Disord Drug Targets. 2010 Apr. 9(2):132-9. [QxMD MEDLINE Link].
Goldman JS, Hahn SE, Catania JW, LaRusse-Eckert S, Butson MB, Rumbaugh M, et al. Genetic counseling and testing for Alzheimer disease: joint practice guidelines of the American College of Medical Genetics and the National Society of Genetic Counselors. Genet Med. 2011 Jun. 13(6):597-605. [QxMD MEDLINE Link]. [Full Text].
Hollingworth P, Harold D, Sims R, et al. Common variants at ABCA7, MS4A6A/MS4A4E, EPHA1, CD33 and CD2AP are associated with Alzheimer's disease. Nat Genet. 2011 May. 43(5):429-35. [QxMD MEDLINE Link]. [Full Text].
Caselli RJ, Dueck AC. APOE varepsilon2 and presymptomatic stage Alzheimer disease: how much is not enough?. Neurology. 2010 Nov 30. 75(22):1952-3. [QxMD MEDLINE Link].
Chiang GC, Insel PS, Tosun D, et al. Hippocampal atrophy rates and CSF biomarkers in elderly APOE2 normal subjects. Neurology. 2010 Nov 30. 75(22):1976-81. [QxMD MEDLINE Link].
Finch CE, Morgan TE. Systemic inflammation, infection, ApoE alleles, and Alzheimer disease: a position paper. Curr Alzheimer Res. 2007 Apr. 4(2):185-9. [QxMD MEDLINE Link].
Anderson P. Hypertension Interacts With APOE Epsilon 4 to Increase Amyloid Load. Available at http://www.medscape.com/viewarticle/781430. Accessed: April 8, 2013.
Rodrigue KM, Rieck JR, Kennedy KM, Devous MD, Diaz-Arrastia R, Park DC. Risk Factors for ß-Amyloid Deposition in Healthy Aging: Vascular and Genetic Effects. JAMA Neurol. 2013 Mar 18. 1-7. [QxMD MEDLINE Link].
Cacciottolo M, Wang X, Driscoll I, Woodward N, Saffari A, Reyes J, et al. Particulate air pollutants, APOE alleles and their contributions to cognitive impairment in older women and to amyloidogenesis in experimental models. Transl Psychiatry. 2017 Jan 31. 7 (1):e1022. [QxMD MEDLINE Link].
Baker LD, Cross DJ, Minoshima S, Belongia D, Watson GS, Craft S. Insulin resistance and Alzheimer-like reductions in regional cerebral glucose metabolism for cognitively normal adults with prediabetes or early type 2 diabetes. Arch Neurol. 2011 Jan. 68(1):51-7. [QxMD MEDLINE Link].
Schrijvers JCM, Witteman EJG, Sijbrands, et al. Insulin metabolism and the risk of Alzheimer disease: The Rotterdam Study. Neurology. 2010;75:1982-1987.
Miklossy J. Emerging roles of pathogens in Alzheimer disease. Expert Rev Mol Med. 2011 Sep 20. 13:e30. [QxMD MEDLINE Link].
Saczynski JS, Beiser A, Seshadri S, Auerbach S, Wolf PA, Au R. Depressive symptoms and risk of dementia: the Framingham Heart Study. Neurology. 2010 Jul 6. 75(1):35-41. [QxMD MEDLINE Link]. [Full Text].
Dotson VM, Beydoun MA, Zonderman AB. Recurrent depressive symptoms and the incidence of dementia and mild cognitive impairment. Neurology. Jul 6 2010. 75(1):27-34.
Lowry F. Late-life depression linked to increased risk for dementia. Medscape Medical News. May 7, 2013. [Full Text].
Diniz BS, Butters MA, Albert SM, Dew MA, Reynolds CF 3rd. Late-life depression and risk of vascular dementia and Alzheimer's disease: systematic review and meta-analysis of community-based cohort studies. Br J Psychiatry. 2013 May. 202:329-35. [QxMD MEDLINE Link]. [Full Text].
Magnoni S, Brody DL. New perspectives on amyloid-beta dynamics after acute brain injury: moving between experimental approaches and studies in the human brain. Arch Neurol. 2010 Sep. 67(9):1068-73. [QxMD MEDLINE Link]. [Full Text].
Chen XH, Siman R, Iwata A, Meaney DF, Trojanowski JQ, Smith DH. Long-term accumulation of amyloid-beta, beta-secretase, presenilin-1, and caspase-3 in damaged axons following brain trauma. Am J Pathol. 2004 Aug. 165(2):357-71. [QxMD MEDLINE Link]. [Full Text].
Plassman BL, Havlik RJ, Steffens DC, Helms MJ, Newman TN, Drosdick D, et al. Documented head injury in early adulthood and risk of Alzheimer's disease and other dementias. Neurology. 2000 Oct 24. 55(8):1158-66. [QxMD MEDLINE Link].
Basha MR, Wei W, Bakheet SA, Benitez N, Siddiqi HK, Ge YW, et al. The fetal basis of amyloidogenesis: exposure to lead and latent overexpression of amyloid precursor protein and beta-amyloid in the aging brain. J Neurosci. 2005 Jan 26. 25(4):823-9. [QxMD MEDLINE Link].
Dizdaroglu M, Jaruga P, Birincioglu M, Rodriguez H. Free radical-induced damage to DNA: mechanisms and measurement. Free Radic Biol Med. 2002 Jun 1. 32(11):1102-15. [QxMD MEDLINE Link].
Harman, D. (1956). Aging: a theory based on free radical and radiation chemistry. J Gerontol. 11, 298-300.
Genin E, Hannequin D, Wallon D, et al. APOE and Alzheimer disease: a major gene with semi-dominant inheritance. Mol Psychiatry. 2011 Sep. 16(9):903-7. [QxMD MEDLINE Link]. [Full Text].
Kochanek KD, Murphy SL, Xu J, Tejada-Vera B. Deaths: Final data for 2014. National Vital Statistics Reports. June 30, 2016. Available at https://www.cdc.gov/nchs/data/nvsr/nvsr65/nvsr65_04.pdf.
Heron M. Deaths: Leading Causes for 2014. National Vital Statistics Reports. June 30, 2016. Available at https://www.cdc.gov/nchs/data/nvsr/nvsr65/nvsr65_05.pdf.
Ives DG, Samuel P, Psaty BM, Kuller LH. Agreement between nosologist and Cardiovascular Health Study review of deaths: Implications of coding differences. Journal of the American Geriatrics Society. 2009. 57:133-139.
Mathers C., Leonardi M. Global burden of dementia in the year 2000:summary of methods and data sources. [Full Text].
Savva GM, Wharton SB, Ince PG, Forster G, Matthews FE, Brayne C. Age, neuropathology, and dementia. N Engl J Med. 2009 May 28. 360(22):2302-9. [QxMD MEDLINE Link]. [Full Text].
Plassman BL, Langa KM, Fisher GG, et al. Prevalence of dementia in the United States: the aging, demographics, and memory study. Neuroepidemiology. 2007. 29(1-2):125-32.
Payami H, Zareparsi S, Montee KR, et al. Gender difference in apolipoprotein E-associated risk for familial Alzheimer disease: a possible clue to the higher incidence of Alzheimer disease in women. Am J Hum Genet. 1996 Apr. 58(4):803-11. [QxMD MEDLINE Link]. [Full Text].
Morris J, Schindler S, McCue L, et al. Assessment of Racial Disparities in Biomarkers for Alzheimer Disease. Jama Neurol. 2019 Jan 7.
Jack CR Jr, Albert MS, Knopman DS, McKhann GM, Sperling RA, Carrillo MC, et al. Introduction to the recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011 May. 7(3):257-62. [QxMD MEDLINE Link]. [Full Text].
Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, et al. Toward defining the preclinical stages of Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011 May. 7(3):280-92. [QxMD MEDLINE Link].
Albert MS, Dekosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, et al. The diagnosis of mild cognitive impairment due to Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011 May. 7(3):270-9. [QxMD MEDLINE Link].
McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR Jr, Kawas CH, et al. The diagnosis of dementia due to Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011 May. 7(3):263-9. [QxMD MEDLINE Link].
American Psychiatric Association. Neurocognitive Disorders. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Washington, DC: American Psychiatric Association; 2013. 611-614.
Teng E, Ringman JM, Ross LK, et al. Diagnosing depression in Alzheimer disease with the national institute of mental health provisional criteria. Am J Geriatr Psychiatry. 2008 Jun. 16(6):469-77. [QxMD MEDLINE Link]. [Full Text].
Lakhan SE, Kirchgessner A. Chronic traumatic encephalopathy: the dangers of getting "dinged". Springerplus. 2012. 1:2. [QxMD MEDLINE Link].
Omalu BI, DeKosky ST, Minster RL, Kamboh MI, Hamilton RL, Wecht CH. Chronic traumatic encephalopathy in a National Football League player. Neurosurgery. 2005 Jul. 57(1):128-34; discussion 128-34. [QxMD MEDLINE Link].
Annweiler C, Schott AM, Allali G, Bridenbaugh SA, Kressig RW, Allain P, et al. Association of vitamin D deficiency with cognitive impairment in older women: cross-sectional study. Neurology. 2010 Jan 5. 74(1):27-32. [QxMD MEDLINE Link].
Buell JS, Dawson-Hughes B, Scott TM, Weiner DE, Dallal GE, Qui WQ, et al. 25-Hydroxyvitamin D, dementia, and cerebrovascular pathology in elders receiving home services. Neurology. 2010 Jan 5. 74(1):18-26. [QxMD MEDLINE Link]. [Full Text].
Chen G, Ward BD, Xie C, Li W, Wu Z, Jones JL, et al. Classification of Alzheimer Disease, Mild Cognitive Impairment, and Normal Cognitive Status with Large-Scale Network Analysis Based on Resting-State Functional MR Imaging. Radiology. 2011 Apr. 259(1):213-21. [QxMD MEDLINE Link]. [Full Text].
Petrella JR, Sheldon FC, Prince SE, Calhoun VD, Doraiswamy PM. Default mode network connectivity in stable vs progressive mild cognitive impairment. Neurology. 2011 Feb 8. 76(6):511-7. [QxMD MEDLINE Link]. [Full Text].
Brooks M. MRI may offer noninvasive option for Alzheimer’s Diagnosis. Medscape Medical News. Dec 27 2012. Available at http://www.medscape.com/viewarticle/776766. Accessed: Jan 8 2012.
McMillan CT, Avants B, Irwin DJ, Toledo JB, et al. Can MRI screen for CSF biomarkers in neurodegenerative disease?. Neurology. 2012 Dec 26. [QxMD MEDLINE Link].
Brooks M. Functional Brain Imaging May Spot Alzheimer's Early. Medscape Medical News. Aug 21 2013. [Full Text].
Wang L, Brier MR, Snyder AZ, et al. Cerebrospinal fluid Aß42, phosphorylated tau181, and resting-state functional connectivity. JAMA Neurol. 2013 Aug 19. [QxMD MEDLINE Link].
Rabinovici GD, Furst AJ, O'Neil JP, Racine CA, Mormino EC, Baker SL, et al. 11C-PIB PET imaging in Alzheimer disease and frontotemporal lobar degeneration. Neurology. 2007 Apr 10. 68(15):1205-12. [QxMD MEDLINE Link].
Anderson, P. New Guidelines for Amyloid PET Imaging. Available at http://www.medscape.com/viewarticle/778274. Accessed: February 5, 2013.
Choi SR, Schneider JA, Bennett DA, Beach TG, Bedell BJ, Zehntner SP, et al. Correlation of amyloid PET ligand florbetapir F 18 binding with Aß aggregation and neuritic plaque deposition in postmortem brain tissue. Alzheimer Dis Assoc Disord. 2012 Jan. 26(1):8-16. [QxMD MEDLINE Link]. [Full Text].
Clark CM, Schneider JA, Bedell BJ, Beach TG, Bilker WB, Mintun MA, et al. Use of florbetapir-PET for imaging beta-amyloid pathology. JAMA. 2011 Jan 19. 305(3):275-83. [QxMD MEDLINE Link].
Fleisher AS, Chen K, Liu X, Roontiva A, Thiyyagura P, Ayutyanont N, et al. Using positron emission tomography and florbetapir F18 to image cortical amyloid in patients with mild cognitive impairment or dementia due to Alzheimer disease. Arch Neurol. 2011 Nov. 68(11):1404-11. [QxMD MEDLINE Link].
Choi SR, Schneider JA, Bennett DA, Beach TG, Bedell BJ, Zehntner SP, et al. Correlation of amyloid PET ligand florbetapir F 18 binding with Aß aggregation and neuritic plaque deposition in postmortem brain tissue. Alzheimer Dis Assoc Disord. 2012 Jan. 26(1):8-16. [QxMD MEDLINE Link]. [Full Text].
Clark CM, Schneider JA, Bedell BJ, Beach TG, Bilker WB, Mintun MA, et al. Use of florbetapir-PET for imaging beta-amyloid pathology. JAMA. 2011 Jan 19. 305(3):275-83. [QxMD MEDLINE Link].
Fleisher AS, Chen K, Liu X, Roontiva A, Thiyyagura P, Ayutyanont N, et al. Using positron emission tomography and florbetapir F18 to image cortical amyloid in patients with mild cognitive impairment or dementia due to Alzheimer disease. Arch Neurol. 2011 Nov. 68(11):1404-11. [QxMD MEDLINE Link].
US Food and Drug Administration (FDA). FDA approves second brain imaging drug to help evaluate patients for Alzheimer’s disease, dementia [press release]. October 25, 2013. Available at http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm372261.htm. Accessed: October 25, 2013.
Neuraceq (florbetaben F 18) prescribing information. [package insert]. Matran Switzerland: Piramal Imaging, S.A. 2014.
Brooks M. Memory tests plus brain scans detect earliest stages of AD. Medscape Medical News. July 15, 2013. [Full Text].
Cassels C. FDA Clears Diagnostic Test for Early Alzheimer's. Medscape Medical News. Available at https://www.medscape.com/viewarticle/973451. May 4, 2022; Accessed: May 9, 2022.
Rasmussen KL, Tybjaerg-Hansen A, Nordestgaard BG, Frikke-Schmidt R. Apolipoprotein E plasma level and genotype -- risk of dementia in 76,000 individuals from the general population. Presented at: XXI World Congress of Neurology (WNC), 2013; September 24, 2013; Vienna, Austria. [Full Text].
Keller DM. APOE plasma levels predict dementia independent of genotype. Medscape Medical News. October 4, 2013. [Full Text].
Green RC, Roberts JS, Cupples LA, et al. Disclosure of APOE genotype for risk of Alzheimer's disease. N Engl J Med. 2009 Jul 16. 361(3):245-54. [QxMD MEDLINE Link]. [Full Text].
Vaz M, Silva V, Monteiro C, Silvestre S. Role of Aducanumab in the Treatment of Alzheimer's Disease: Challenges and Opportunities. Clin Interv Aging. 2022. 17:797-810. [QxMD MEDLINE Link]. [Full Text].
van Dyck CH, Swanson CJ, Aisen P, Bateman RJ, Chen C, Gee M, et al. Lecanemab in Early Alzheimer's Disease. N Engl J Med. 2023 Jan 5. 388 (1):9-21. [QxMD MEDLINE Link].
Salomone S, Caraci F, Leggio GM, Fedotova J, Drago F. New pharmacological strategies for treatment of Alzheimer's disease: focus on disease-modifying drugs. Br J Clin Pharmacol. 2011 Oct 28. [QxMD MEDLINE Link].
Anderson P. Finally, a Winner for Alzheimer's? Antiamyloid Agent Shows Promise. Medscape Medical News. Available at https://www.medscape.com/viewarticle/899841. July 26, 2018; Accessed: July 26, 2018.
Kavanagh S, Gaudig M, Van Baelen B, et al. Galantamine and behavior in Alzheimer disease: analysis of four trials. Acta Neurol Scand. 2011 Nov. 124(5):302-8. [QxMD MEDLINE Link].
Farlow M, Veloso F, Moline M, et al. Safety and tolerability of donepezil 23 mg in moderate to severe Alzheimer's disease. BMC Neurol. 2011 May 25. 11:57. [QxMD MEDLINE Link]. [Full Text].
Starr JM. Cholinesterase inhibitor treatment and urinary incontinence in Alzheimer's disease. J Am Geriatr Soc. 2007 May. 55(5):800-1. [QxMD MEDLINE Link].
Gill SS, Anderson GM, Fischer HD, Bell CM, Li P, Normand SL, et al. Syncope and its consequences in patients with dementia receiving cholinesterase inhibitors: a population-based cohort study. Arch Intern Med. 2009 May 11. 169(9):867-73. [QxMD MEDLINE Link].
Aduhelm (aducanumab) [package insert]. Cambridge, MA: Biogen Inc. June 2021. Available at [Full Text].
Kuller LH, Lopez OL. ENGAGE and EMERGE: Truth and consequences?. Alzheimers Dement. 2021 Apr. 17 (4):692-695. [QxMD MEDLINE Link].
Brauser D. FDA Leader Explains Rationale Leading to Controversial Alzheimer's Drug Approval. Medscape Medical News. Available at https://www.medscape.com/viewarticle/953618. June 23, 2021; Accessed: July 20, 2021.
Abbott A. Could drugs prevent Alzheimer's? These trials aim to find out. Nature. 2022 Mar. 603 (7900):216-219. [QxMD MEDLINE Link]. [Full Text].
Lachaine J, Beauchemin C, Legault M, Bineau S. Economic evaluation of the impact of memantine on time to nursing home admission in the treatment of Alzheimer disease. Can J Psychiatry. 2011 Oct. 56(10):596-604. [QxMD MEDLINE Link].
Schmitt FA, van Dyck CH, Wichems CH, Olin JT. Cognitive response to memantine in moderate to severe Alzheimer disease patients already receiving donepezil: an exploratory reanalysis. Alzheimer Dis Assoc Disord. 2006 Oct-Dec. 20(4):255-62. [QxMD MEDLINE Link].
Porsteinsson AP, Grossberg GT, Mintzer J, Olin JT. Memantine treatment in patients with mild to moderate Alzheimer's disease already receiving a cholinesterase inhibitor: a randomized, double-blind, placebo-controlled trial. Curr Alzheimer Res. 2008 Feb. 5(1):83-9. [QxMD MEDLINE Link].
Schneider LS, Dagerman KS, Higgins JP, McShane R. Lack of evidence for the efficacy of memantine in mild Alzheimer disease. Arch Neurol. 2011 Aug. 68(8):991-8. [QxMD MEDLINE Link].
Greig SL. Memantine ER/Donepezil: A Review in Alzheimer's Disease. CNS Drugs. 2015 Nov. 29 (11):963-70. [QxMD MEDLINE Link].
Jeffrey S. FDA Approves Exelon Patch for Severe Alzheimer's. Medscape [serial online]. Available at http://www.medscape.com/viewarticle/807062. Accessed: July 8, 2013.
Farlow MR, Grossberg G, Gauthier S, Meng X, Olin JT. The ACTION study: methodology of a trial to evaluate safety and efficacy of a higher dose rivastigmine transdermal patch in severe Alzheimer's disease. Curr Med Res Opin. 2010 Oct. 26(10):2441-7. [QxMD MEDLINE Link].
de Rotrou J, Cantegreil I, Faucounau V, et al. Do patients diagnosed with Alzheimer's disease benefit from a psycho-educational programme for family caregivers? A randomised controlled study. Int J Geriatr Psychiatry. 2011 Aug. 26(8):833-42. [QxMD MEDLINE Link].
Deaths with Antipsychotics in Elderly Patients with Behavioral Disturbances. US Food and Drug Administration Website. Available at http://www.fda.gov/Drugs/DrugSafety/PublicHealthAdvisories/ucm053171.htm. Accessed: August 11, 2009.
Devanand DP, Pelton GH, Cunqueiro K, Sackeim HA, Marder K. A 6-month, randomized, double-blind, placebo-controlled pilot discontinuation trial following response to haloperidol treatment of psychosis and agitation in Alzheimer's disease. Int J Geriatr Psychiatry. 2011 Sep. 26(9):937-43. [QxMD MEDLINE Link].
Vigen CL, Mack WJ, Keefe RS, et al. Cognitive effects of atypical antipsychotic medications in patients with Alzheimer's disease: outcomes from CATIE-AD. Am J Psychiatry. 2011 Aug. 168(8):831-9. [QxMD MEDLINE Link].
Nyth AL, Gottfries CG. The clinical efficacy of citalopram in treatment of emotional disturbances in dementia disorders. A Nordic multicentre study. Br J Psychiatry. 1990 Dec. 157:894-901. [QxMD MEDLINE Link].
US Food and Drug Administration. August 24, 2011. FDA Drug Safety Communication: Abnormal heart rhythms associated with high doses of Celexa (citalopram hydrobromide). Available at http://www.fda.gov/Drugs/DrugSafety/ucm269086.htm. Accessed: December 27, 2011.
Porsteinsson AP, Drye LT, Pollock BG, Devanand DP, Frangakis C, Ismail Z, et al. Effect of citalopram on agitation in Alzheimer disease: the CitAD randomized clinical trial. JAMA. 2014 Feb 19. 311(7):682-91. [QxMD MEDLINE Link].
Small GW. Treating dementia and agitation. JAMA. 2014 Feb 19. 311(7):677-8. [QxMD MEDLINE Link].
Anderson P. Citalopram Reduces Agitation in Patients With Alzheimer's. Medscape Medical News. Available at http://www.medscape.com/viewarticle/820741. Accessed: February 24, 2014.
Weintraub D, Rosenberg PB, Drye LT, et al. Sertraline for the treatment of depression in Alzheimer disease: week-24 outcomes. Am J Geriatr Psychiatry. 2010 Apr. 18(4):332-40. [QxMD MEDLINE Link]. [Full Text].
Petracca GM, Chemerinski E, Starkstein SE. A double-blind, placebo-controlled study of fluoxetine in depressed patients with Alzheimer's disease. Int Psychogeriatr. 2001 Jun. 13(2):233-40. [QxMD MEDLINE Link].
Banerjee S, Hellier J, Dewey M, et al. Sertraline or mirtazapine for depression in dementia (HTA-SADD): a randomised, multicentre, double-blind, placebo-controlled trial. Lancet. 2011 Jul 30. 378(9789):403-11. [QxMD MEDLINE Link].
Boggs W. Trazodone Treats Sleep Disturbance in Alzheimer's Disease. Medscape Medical News. Available at http://www.medscape.com/viewarticle/819383. Accessed: January 26, 2014.
Camargos E, Louzada L, Quintas J, Naves J, Louzada F, Nóbrega O. Trazodone improves sleep parameters in Alzheimer's disease patients: a randomized, double-blind and placebo-controlled study. Am J Geriatr Psychiatry. 2014 Jan 4. [Epub ahead of print].
Tariot PN, Schneider LS, Cummings J, et al. Chronic divalproex sodium to attenuate agitation and clinical progression of Alzheimer disease. Arch Gen Psychiatry. 2011 Aug. 68(8):853-61. [QxMD MEDLINE Link].
Wang YY, Zheng W, Ng CH, Ungvari GS, Wei W, Xiang YT. Meta-analysis of randomized, double-blind, placebo-controlled trials of melatonin in Alzheimer's disease. Int J Geriatr Psychiatry. 2016 Sep 19. [QxMD MEDLINE Link].
Anderson P. 'Z' Drugs Significantly Boost Fracture Risk in Dementia Patients. Medscape Medical News. Available at https://www.medscape.com/viewarticle/899792. July 25, 2018; Accessed: July 30, 2018.
Breitner JC, Haneuse S, Walker R, Dublin S, Crane PK, Gray SL, et al. Risk of dementia and AD with prior exposure to NSAIDs in an elderly community-based cohort. Neurology. Jun 2 2009. 72(22):1899-1905.
Pritchard SM, Dolan PJ, Vitkus A, Johnson GV. The toxicity of tau in Alzheimer disease: turnover, targets and potential therapeutics. J Cell Mol Med. 2011 Aug. 15(8):1621-35. [QxMD MEDLINE Link].
Sano M, Ernesto C, Thomas RG, et al. A controlled trial of selegiline, alpha-tocopherol, or both as treatment for Alzheimer's disease. The Alzheimer's Disease Cooperative Study. N Engl J Med. 1997 Apr 24. 336(17):1216-22. [QxMD MEDLINE Link].
Brooks M. Vitamin E May Slow Functional Decline in Mild Alzheimer's. Medscape Medical News. Available at http://www.medscape.com/viewarticle/818533. Accessed: January 8, 2014.
Dysken MW, Sano M, Asthana S, Vertrees JE, Pallaki M, Llorente M, et al. Effect of vitamin E and memantine on functional decline in Alzheimer disease: the TEAM-AD VA cooperative randomized trial. JAMA. 2014 Jan 1. 311(1):33-44. [QxMD MEDLINE Link].
Sano M, Bell KL, Galasko D, Galvin JE, Thomas RG, van Dyck CH, et al. A randomized, double-blind, placebo-controlled trial of simvastatin to treat Alzheimer disease. Neurology. 2011 Aug 9. 77(6):556-63. [QxMD MEDLINE Link]. [Full Text].
Freitas C, Mondragón-Llorca H, Pascual-Leone A. Noninvasive brain stimulation in Alzheimer's disease: systematic review and perspectives for the future. Exp Gerontol. 2011 Aug. 46(8):611-27. [QxMD MEDLINE Link].
Henderson ST, Vogel JL, Barr LJ, Garvin F, Jones JJ, Costantini LC. Study of the ketogenic agent AC-1202 in mild to moderate Alzheimer's disease: a randomized, double-blind, placebo-controlled, multicenter trial. Nutr Metab (Lond). 2009 Aug 10. 6:31. [QxMD MEDLINE Link]. [Full Text].
Harrison P. Novel Intervention May Reverse Alzheimer's Memory Loss. Medscape Medical News. Available at http://www.medscape.com/viewarticle/832752. Accessed: 10/8/14.
Bredesen D. Reversal of cognitive decline: A novel therapeutic program. Aging. September 2014. [Full Text].
Hörder H, Johansson L, Guo X, Grimby G, Kern S, Östling S, et al. Midlife cardiovascular fitness and dementia: A 44-year longitudinal population study in women. Neurology. 2018 Mar 14. [QxMD MEDLINE Link].
Barberger-Gateau P, Raffaitin C, Letenneur L, Berr C, Tzourio C, Dartigues JF, et al. Dietary patterns and risk of dementia: the Three-City cohort study. Neurology. 2007 Nov 13. 69(20):1921-30. [QxMD MEDLINE Link].
Solfrizzi V, Panza F, Frisardi V, Seripa D, Logroscino G, Imbimbo BP, et al. Diet and Alzheimer's disease risk factors or prevention: the current evidence. Expert Rev Neurother. 2011 May. 11(5):677-708. [QxMD MEDLINE Link].
Witte AV, Fobker M, Gellner R, Knecht S, Flöel A. Caloric restriction improves memory in elderly humans. Proc Natl Acad Sci U S A. 2009 Jan 27. 106(4):1255-60. [QxMD MEDLINE Link]. [Full Text].
Anstey KJ, Mack HA, Cherbuin N. Alcohol consumption as a risk factor for dementia and cognitive decline: meta-analysis of prospective studies. Am J Geriatr Psychiatry. 2009 Jul. 17(7):542-55. [QxMD MEDLINE Link].
Virtaa JJ, Järvenpää T, Heikkilä K, Perola M, Koskenvuo M, Räihä I, et al. Midlife alcohol consumption and later risk of cognitive impairment: a twin follow-up study. J Alzheimers Dis. 2010. 22(3):939-48. [QxMD MEDLINE Link].
Schwarzinger M, Pollock BG, Hasan OSM, Dufouil C, Rehm J, QalyDays Study Group. Contribution of alcohol use disorders to the burden of dementia in France 2008-13: a nationwide retrospective cohort study. Lancet Public Health. 2018 Mar. 3 (3):e124-e132. [QxMD MEDLINE Link].
Brooks M. First Alzheimer's Guidelines for Clinical Practice Released. Medscape Medical News. Available at https://www.medscape.com/viewarticle/899674. July 23, 2018; Accessed: July 30, 2018.
Brooks M. Brain Insulin Resistance Marker May Diagnose Alzheimer's. Medscape Medical News. Available at http://www.medscape.com/viewarticle/835489.. Accessed: November 27, 2014.
Billioti de Gage S, Moride Y, Ducruet T, Kurth T, Verdoux H, Tournier M, et al. Benzodiazepine use and risk of Alzheimer's disease: case-control study. BMJ. 2014 Sep 9. 349:g5205. [QxMD MEDLINE Link]. [Full Text].
Brauser D. Benzodiazepines Linked to Increased Alzheimer's Risk. Medscape Medical News. Available at http://www.medscape.com/viewarticle/831403. Accessed: September 14, 2014.
Cassels C. Simple Eye Tests to Detect Alzheimer's Disease in the Works. Medscape Medical News. Jul 16 2014. [Full Text].
Davenport L. Herpes simplex may double Alzheimer's risk. Medscape Medical New. October 27, 2014. [Full Text].
Dysken MW, Sano M, Asthana S, Vertrees JE, Pallaki M, Llorente M, et al. Effect of vitamin E and memantine on functional decline in Alzheimer disease: the TEAM-AD VA cooperative randomized trial. JAMA. 2014 Jan 1. 311(1):33-44. [QxMD MEDLINE Link].
Hebert LE, Scherr PA, Bienias JL, Bennett DA, Evans DA. Alzheimer disease in the US population: prevalence estimates using the 2000 census. Arch Neurol. 2003 Aug. 60(8):1119-22. [QxMD MEDLINE Link].
Jeffrey S. FDA Approves Third Amyloid PET Tracer for Alzheimer's. Medscape Medical News. Available at http://www.medscape.com/viewarticle/822370. Accessed: March 31, 2014.
Lovheim H, Gilthorpe J, Adolfsson R, Nilsson LG, Elgh F. Reactivated herpes simplex infection increases the risk of Alzheimer's disease. Alzheimers Dement. 2014 Jul 17. [QxMD MEDLINE Link].
Lovheim H, Gilthorpe J, Johansson A, Eriksson S, Hallmans G, Elgh F. Herpes simplex infection and the risk of Alzheimer's disease-A nested case-control study. Alzheimers Dement. 2014 Oct 7. [QxMD MEDLINE Link].
Yaffe K, Boustani M. Benzodiazepines and risk of Alzheimer's disease. BMJ. 2014 Sep 9. 349:g5312. [QxMD MEDLINE Link].

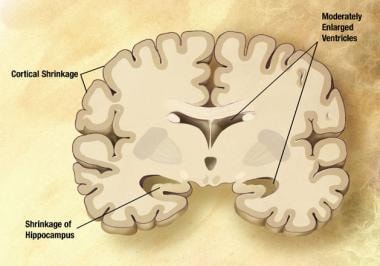 Mild Alzheimer disease. The disease begins to affect the cerebral cortex, memory loss continues, and changes in other cognitive abilities emerge. The clinical diagnosis of AD is usually made during this stage. Image courtesy of NIH.
Mild Alzheimer disease. The disease begins to affect the cerebral cortex, memory loss continues, and changes in other cognitive abilities emerge. The clinical diagnosis of AD is usually made during this stage. Image courtesy of NIH.

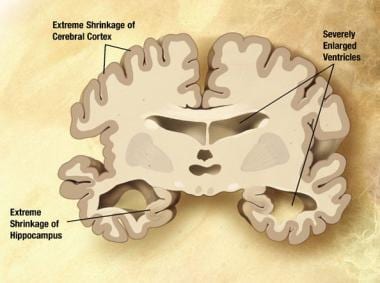 Severe Alzheimer disease. In the last stage of AD, plaques and tangles are widespread throughout the brain, and areas of the brain have atrophied further. Patients cannot recognize family and loved ones or communicate in any way. They are completely dependent on others for care. All sense of self seems to vanish. Image courtesy of NIH.
Severe Alzheimer disease. In the last stage of AD, plaques and tangles are widespread throughout the brain, and areas of the brain have atrophied further. Patients cannot recognize family and loved ones or communicate in any way. They are completely dependent on others for care. All sense of self seems to vanish. Image courtesy of NIH.









